Cerebral Cortex Surgery is a General or Functional Neurosurgery? Lecture by R. García de Sola
Dr. Rafael García de Sola, invited by the Spanish Society of Functional and Stereotactic Neurosurgery (SENFE). Palma de Mallorca (Spain), 2017.
Prof. Dr. Rafael García de Sola
Director de la Cátedra UAM de “Innovación en Neurocirugía”
Facultad de Medicina. Universidad Autónoma de Madrid (UAM)
Good afternoon.
I would like to thank Dr Mónica Lara, the organizer of this Meeting, for inviting me to deliver this Lecture.
It is a great honour.
Cerebral Cortex Surgery: See presentation…
History
Krause
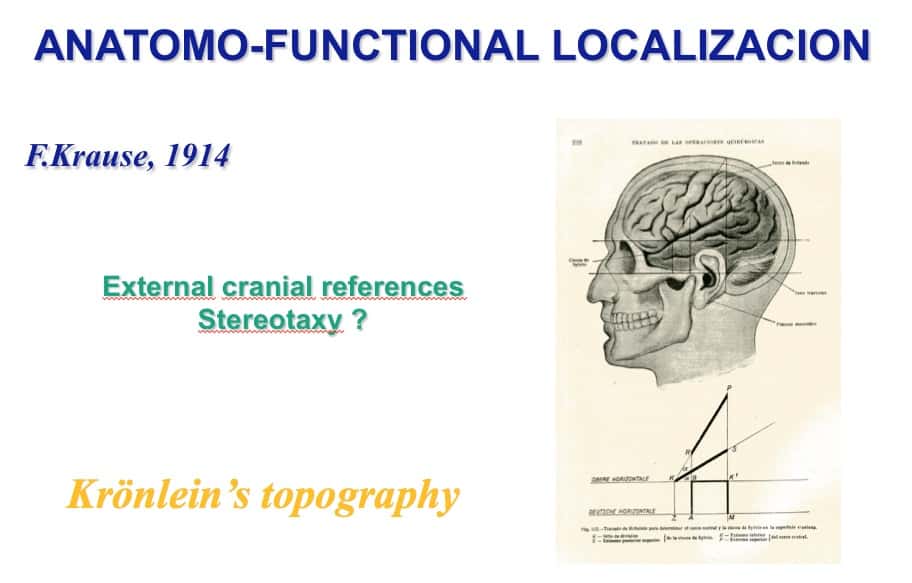
When I was looking through my father’s library, I came across this book by Krause from 1915, more than a century ago.
At the dawn of Neurosurgery.
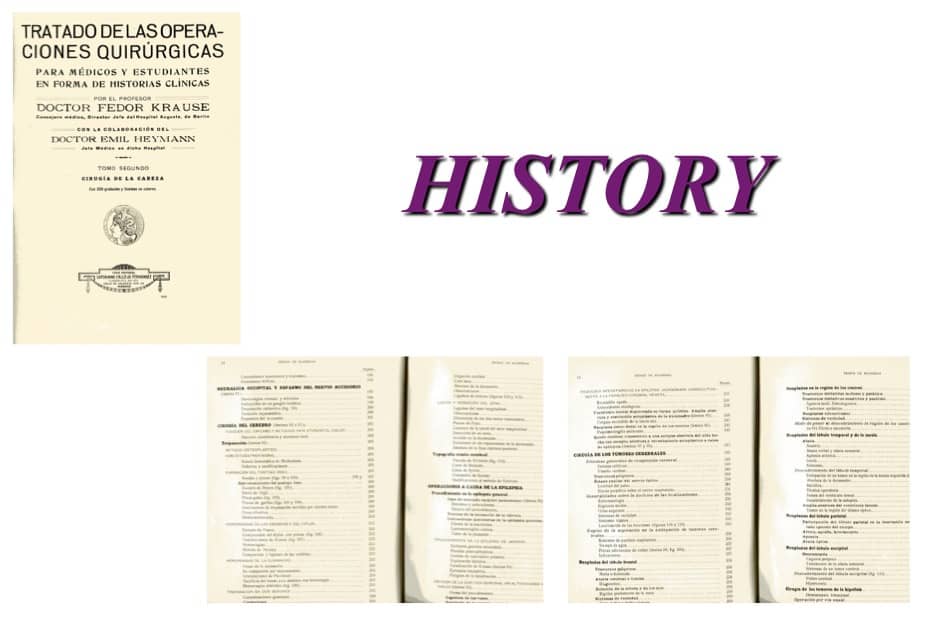
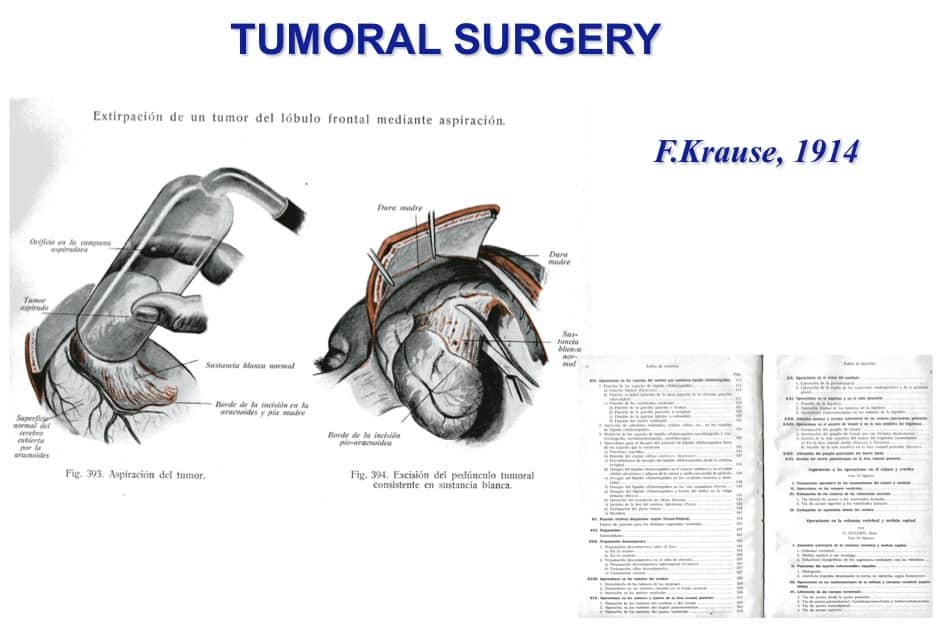
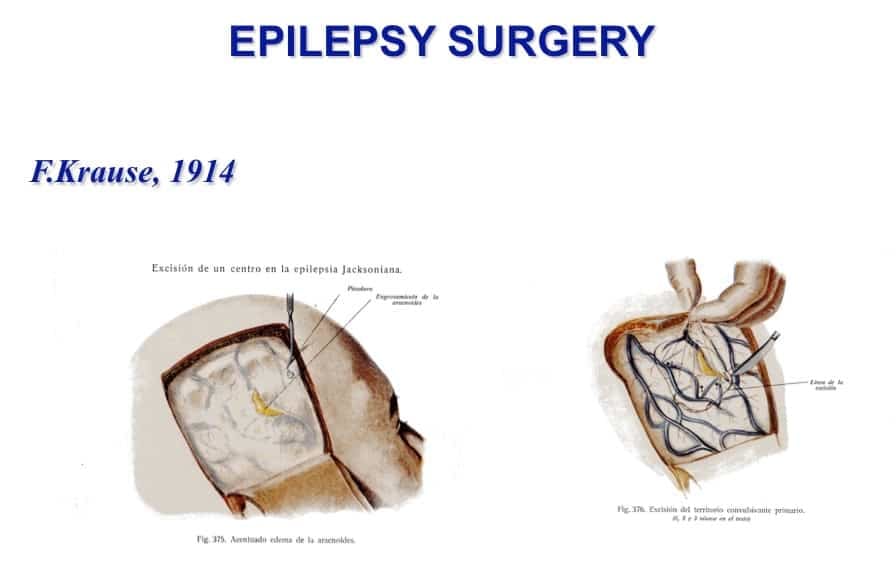
He presented three important chapters. About general neurosurgical principles, tumoral surgery and epilepsy surgery.
From the contents of the first chapter two facts standout.
The first, was his own results with electric faradic cortical stimulacion to locate the function of primary areas.
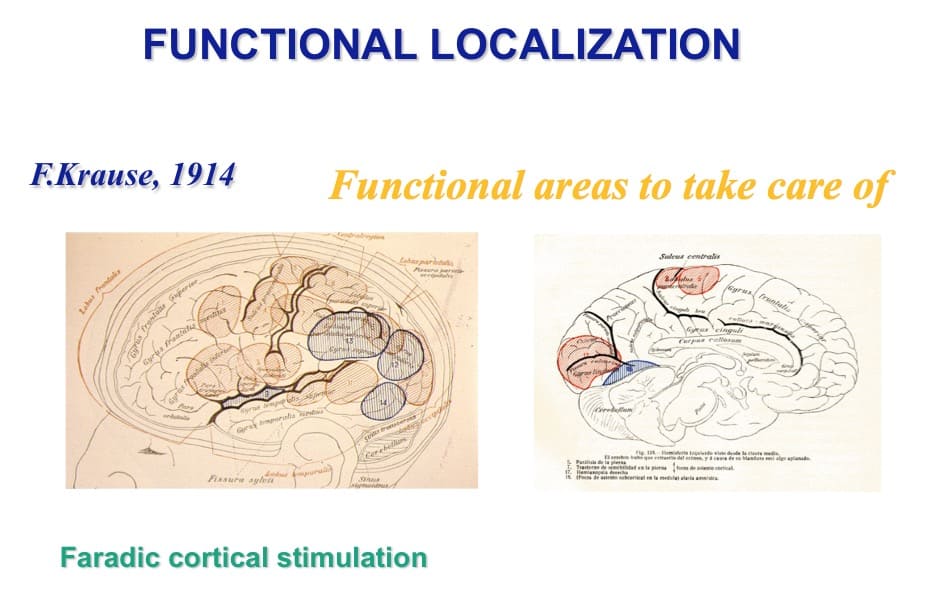
Krönlein
The second was the description of the external references to localize these areas, using Krönlein’s topography.
Could this be considered the birth of stereotaxy?
The second chapter described how to remove cortical tumors, using primitive aspiration technology.
The third chapter was dedicated to epilepsy surgery, almost with the same detail as the previous chapter. With the description of the removal of an epileptic scar.
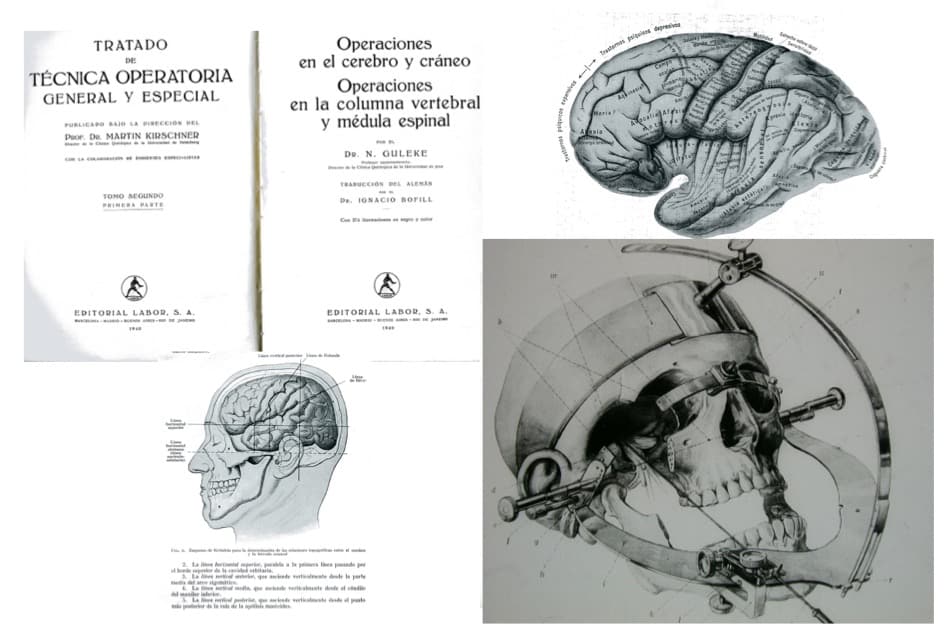
Kirscher
30 years later, in the 1940’s, Kirscher published another book about neurosurgical pathology and techniques. Apparently there have been no advances. Except for certain details as his proposal of using his stereotactic tool to reach the Gasserian ganglion, trough the foramen ovale.
Cerebral Cortex Surgery: Leading figures of the progress
Since then, great progress has been made. And several figures deserve to be mentioned.
From my point of view,
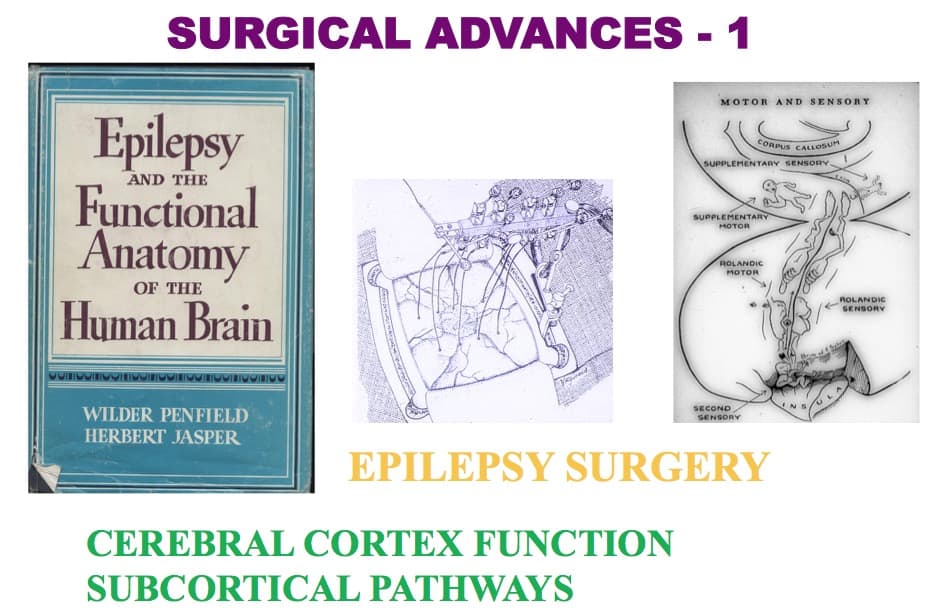
Penfield and Jasper
The fist two were Penfield and Jasper, in the 1940’s. They established a methodology, not only to explore and operate on epileptic patients, but also to explore the cerebral cortex function and the subcortical pathways.
Talairach and Bancaud
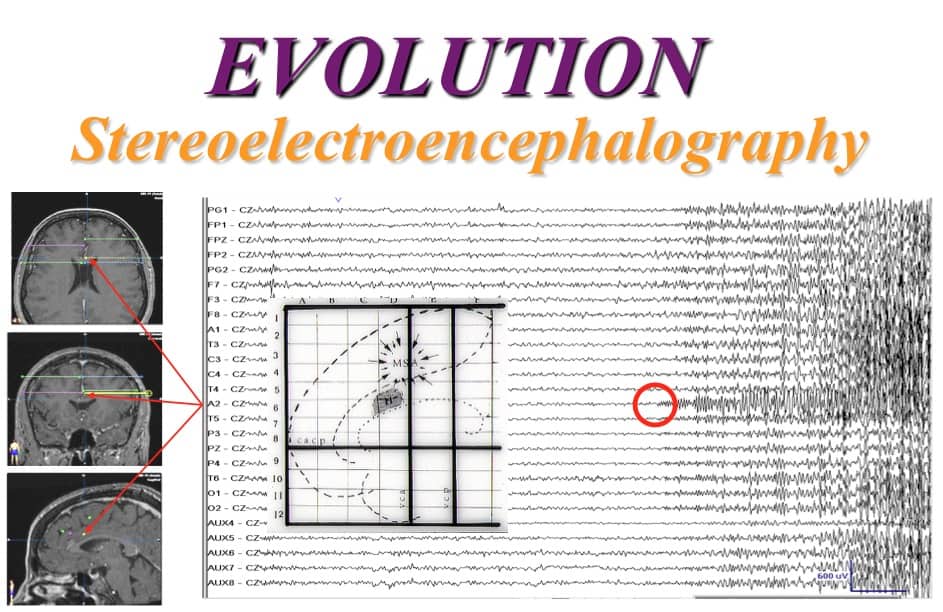
The second two, for me, are Talairach and Bancaud. 20 years later, when they proposed a new methodology of exploring epileptic patient, after implantating depth electrodes. The method was called Stereoelectroencephalography.
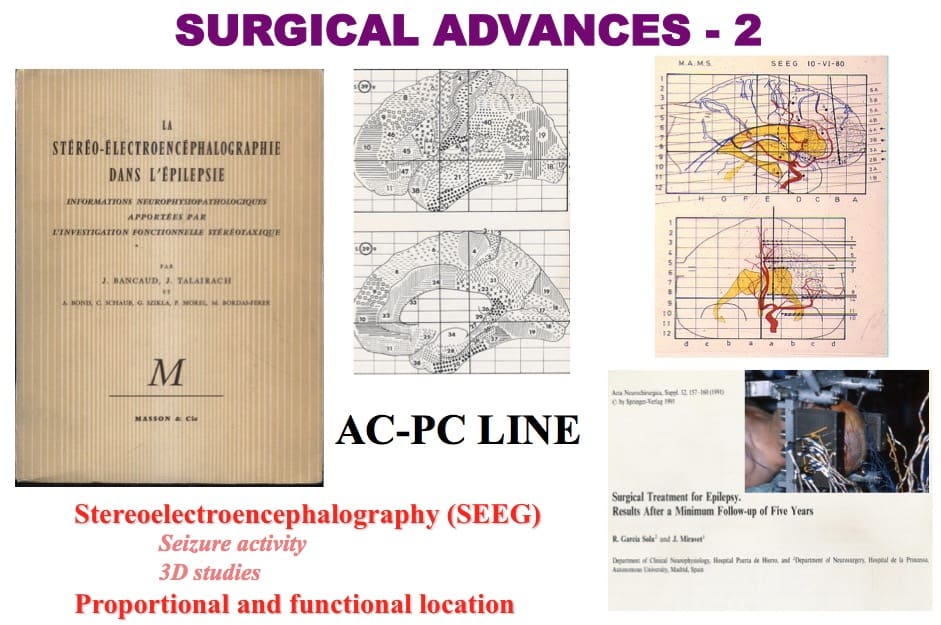
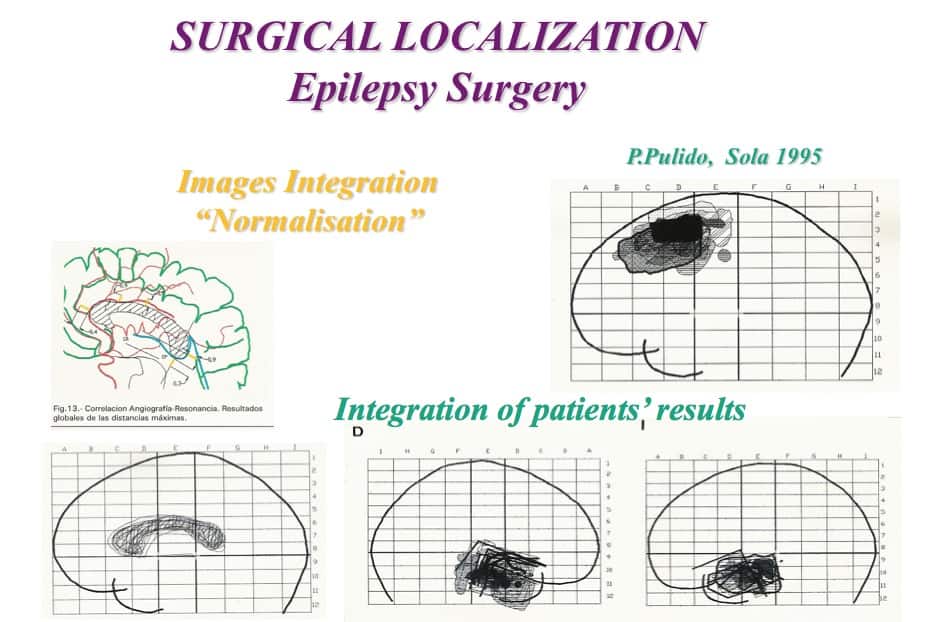
Bedsides this, they suggested drawing individual anatomo-funtional maps, based on the AC-PC line, with the capability of performing a “Normalization” procedure to collet the information of several patients with similar pathology and findings.
In a special operating theatre stablished in Puerta de Hierro Hospital, in Madrid, we followed this Talairach and Bancaud methodology..
I was lucky enough to be the neurosurgeon in charge of this OR, from 1978 to 1983.
In 1990, I moved to the La Princesa Hospital and I began a new program of epilepsy surgery.
Since then, the Department has been recognized as a national reference centre by the Ministry of Health.
Yasargil
The next important figure in the neurosurgical evolution, for me, is Yasargil.
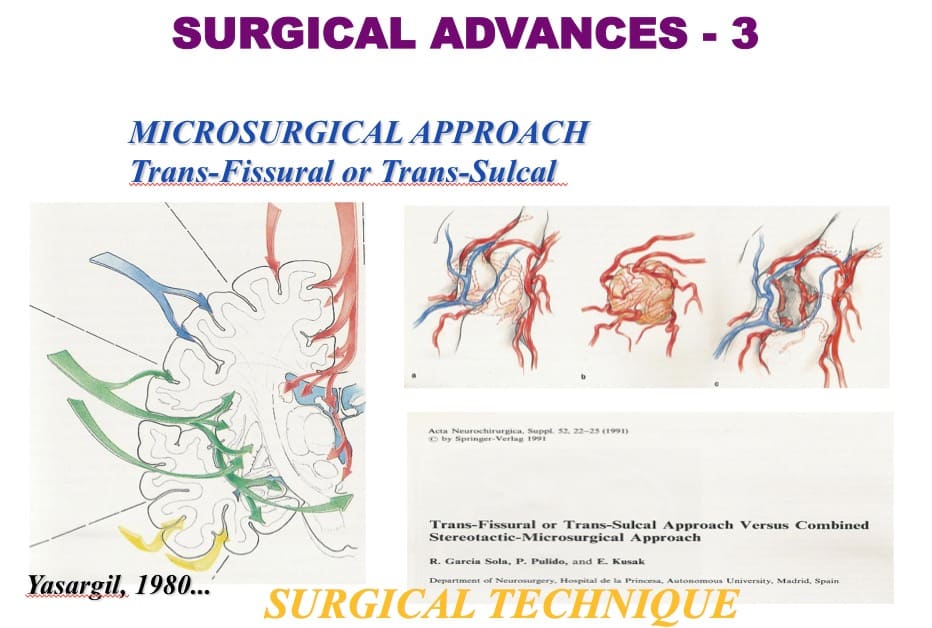
Besides his excellent surgical conception of cerebral cortex,
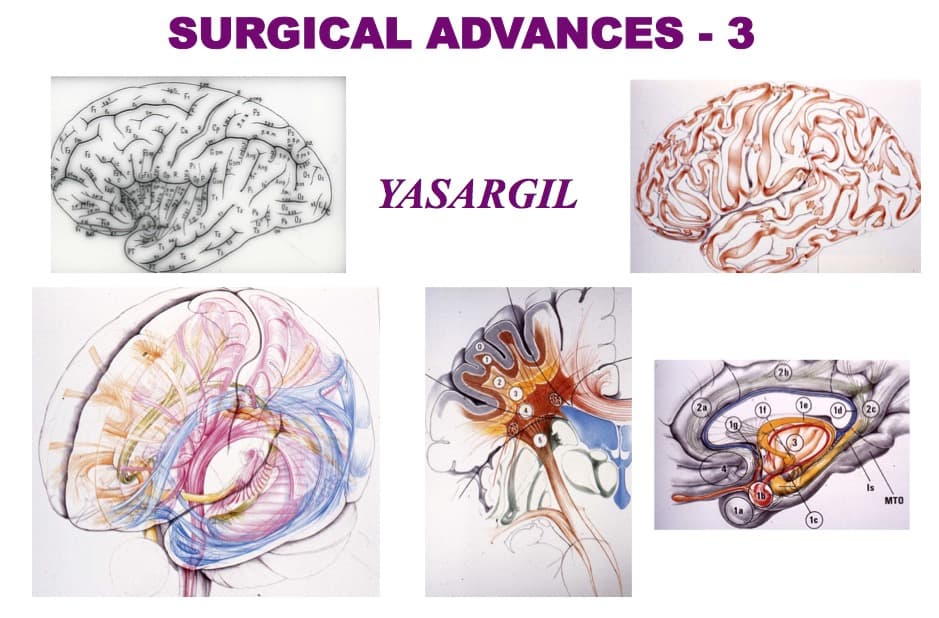
Yasargil proposed a new approach to deep lesions: trans-fissural or trans-sulcal. It was a hugh step forward.
And we adopted this approach.

Cerebral Cortex Surgery: Neuronavigation
Let me move on now to the fourth key fact which has made important progress in Neurosurgery: Neuronavigation.
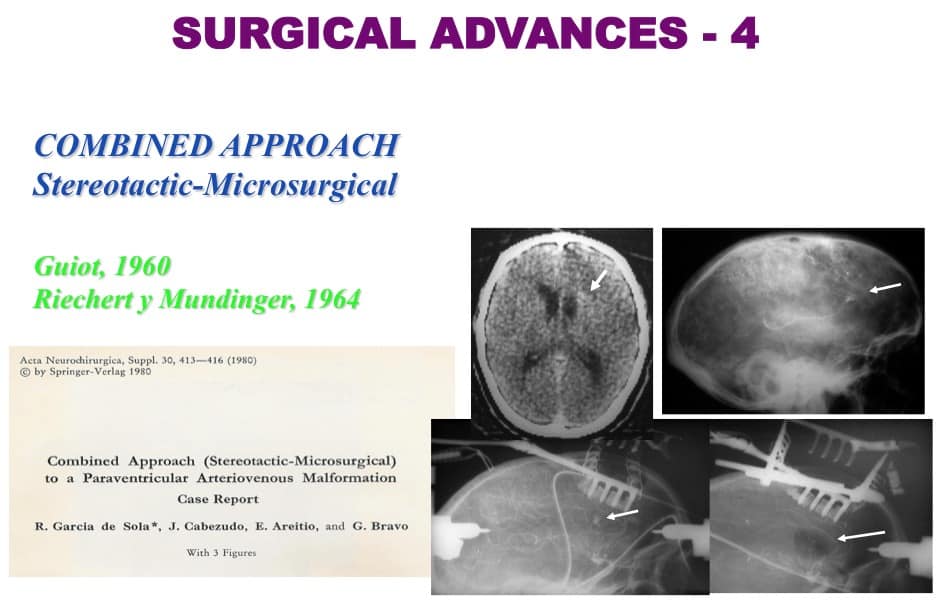
Guiot and Riecher and Mundinguer
At the beginning, the only accurate approach to deep lesions was to take advantage of the stereotactic frame and place a cannula near to the lesion and follow it.
This was proposed by Guiot and Riecher and Mundinguer.
And we were the first neurosurgeons to advise the use of a microscope to reach the tip of the cannula and the lesion.
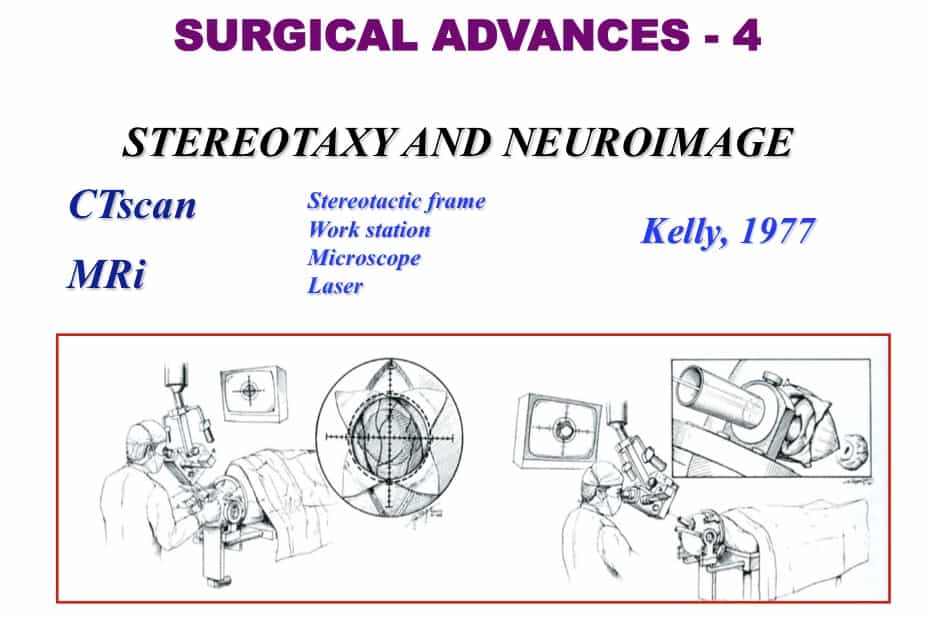
Kelly
In the 1970’s, Kelly proposed a complex method to reach and remove this kinds of lesions.
A combination of a specific stereotactic frame, a workstation with a treating images software, microscope and laser.
It was an original, innovative and unique approach.
And it pointed the way on how to reach deep lesions.
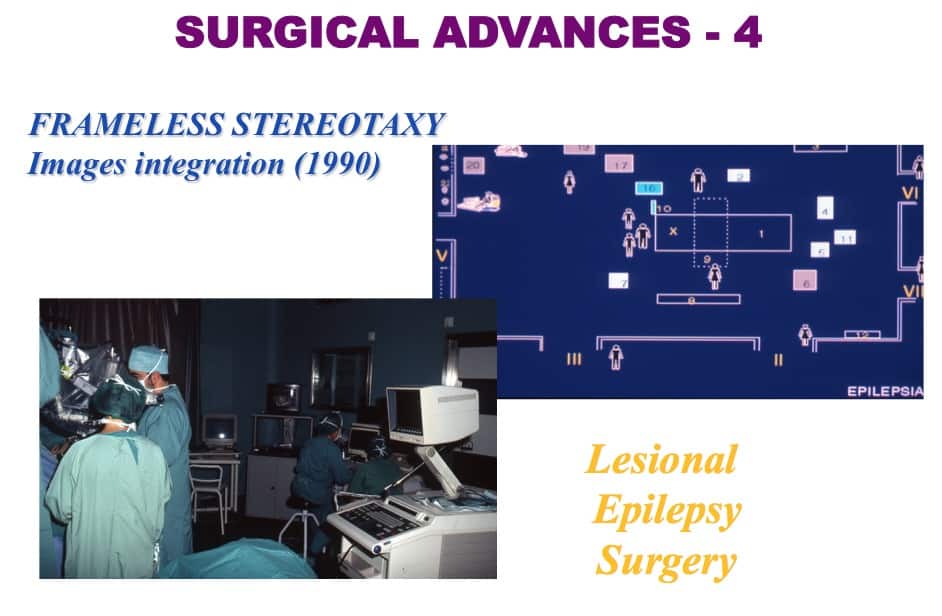
Frameless stereotaxy
In the 1980’s laser technology was fashionable and useful. We had the opportunity to use CO2 and NdYAG laser, integrated through the same microscope.
And we began to use an early neurophysiological intraoperative monitoring technology.
But although we may have had the most sophisticated technology, we still had serious difficulties finding deep lesions.
The dilemma back them was either
- ONE, used the stereotactic-microsurgical approach,
- TWO, used intraoperative ultrasonography.
- THREE, bought the Kelly’s equipment.
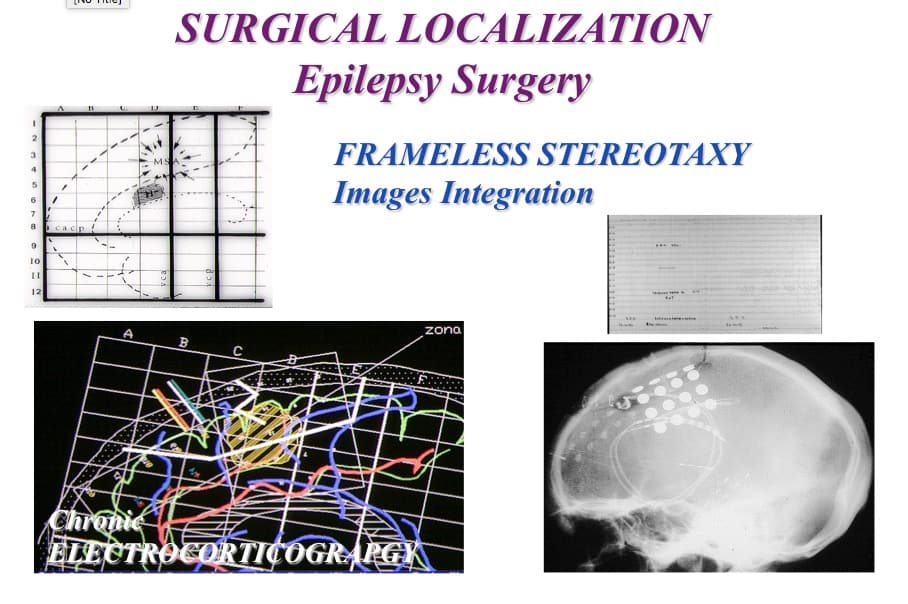
- Or, finally, tried to design another method, according to the latest trend of “frameless stereotaxy”
.
We chose the last option.
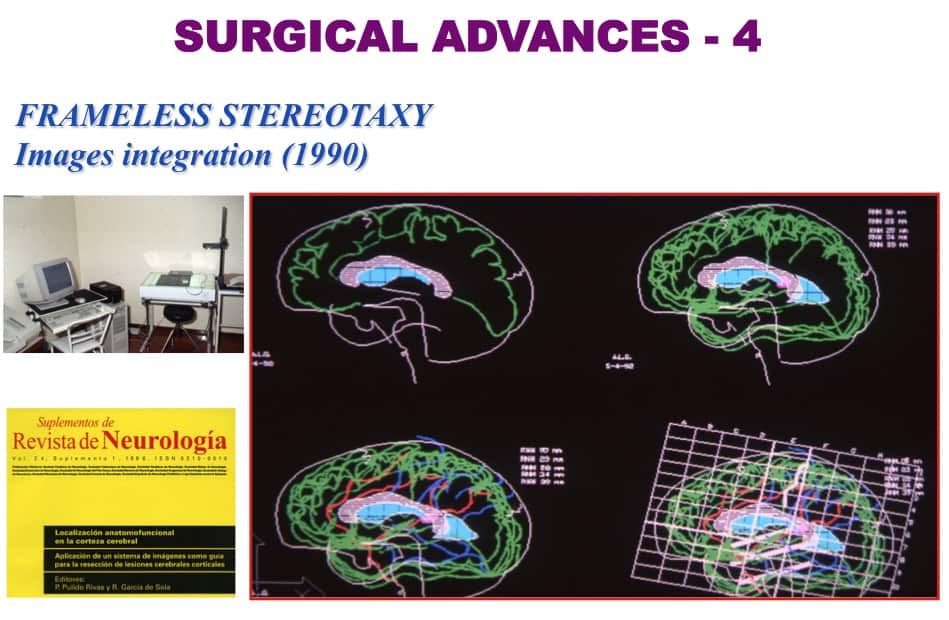
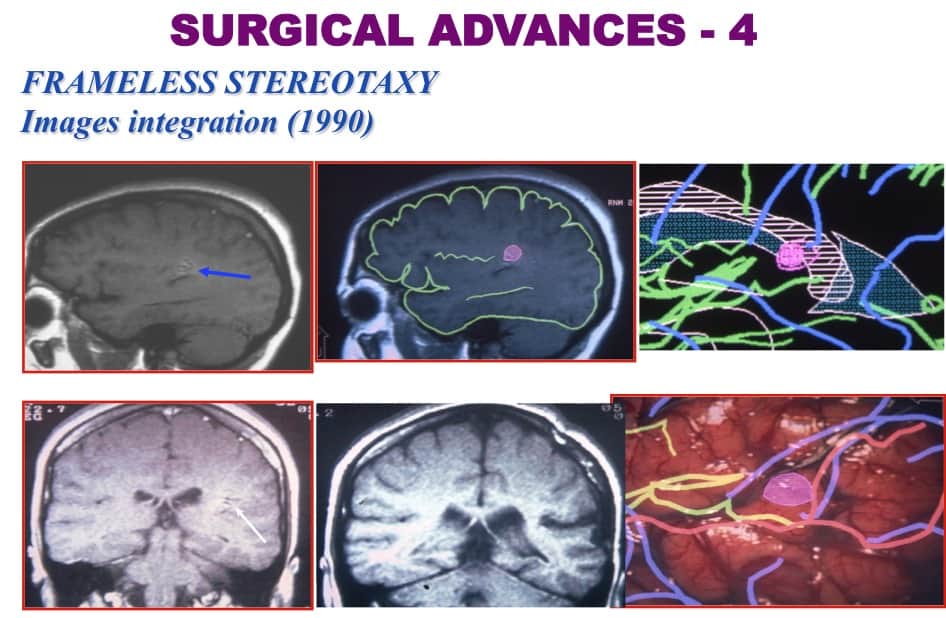
In a workstation, with Autocad software and a transparent digital pad, we could draw the contour of cerebral cortex of the different MRi slides. We could superimposed them on to each other, according to the AC-PC line.
Afterward, we included other layer as the Talairach’s grid or angiography (arteries and veins).
The result was an anatomical map, where it was possible to locate the lesion, the sulcus to reach it and the proximal veins and arteries to be used as anatomical landmarks.
I would like to present one of the most difficult cases encountered.
There was a cavernous angioma, deep to the left supramarginal girus.
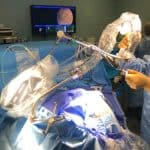
We put the patient’s head sagittal plane parallel to the floor. The microscope was orthogonal to this plane.
In the computer, we superimposed the microscopic view of the surgical field on to the patient’s images.
After identifying the veins, we approached the correct sulcus to reach the lesion and to remove it.
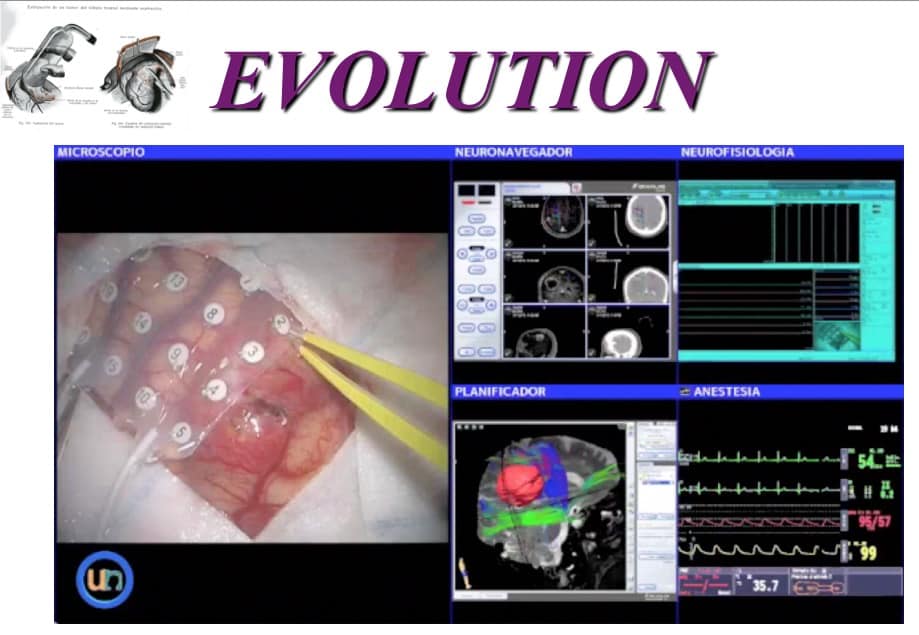
Evolution of the operating room
Finally, the fifth important advance has been the evolution of the operating theatre.
We must always make the effort to adapt the OR to different kinds of surgeries, so it is possible to take a holistic approach.
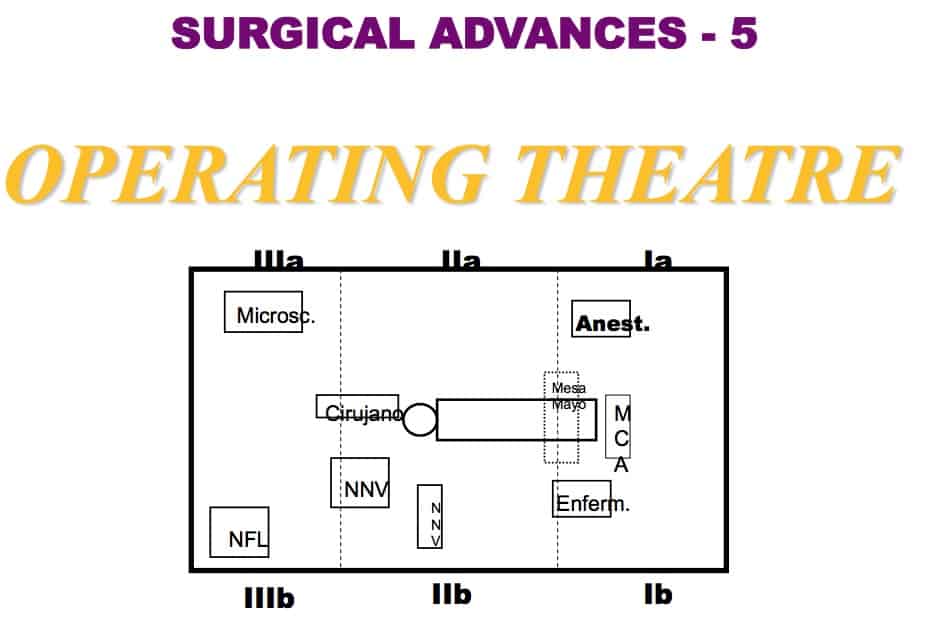
Nevertheless, we have to adapt to new ideas. We have to look to the future. For instances, many people now talk about “intelligent” Operating Room (OR).
And we have incorporated new technological advances into the OR (as robots or endoscopy), and we need to link these together.
But we need also to get more detail data from each operation, and a more complete document of each procedure, that will be also useful for training and research.
Here is a picture of the operating theatre in La Princesa and in el Rosario hospitals.

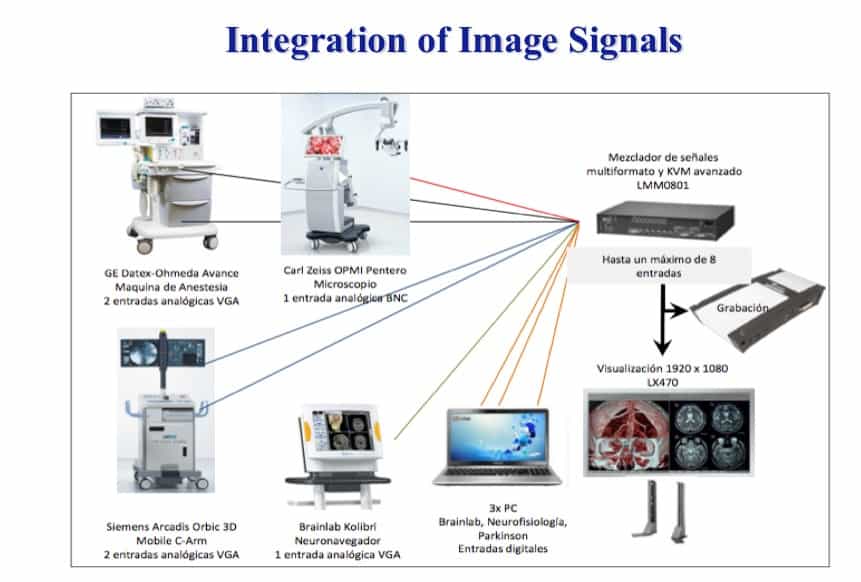
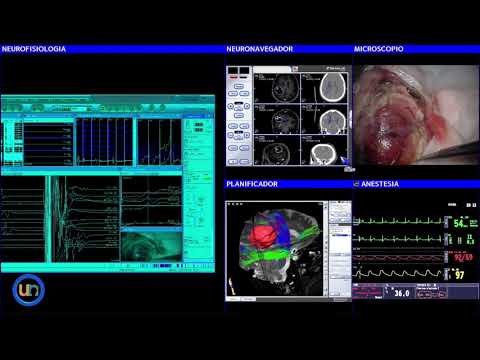
Integration of image signals
To solve this, we have designed an images integration device. It makes it possible to integrate up to 9 signals of different screens: microscope, neuronavigation, neurophysiology, work station, anaesthesia, etc.
Let me finish this first part of this presentation showing you an example of how to reach a deep cavernous angioma, through a transulcal approach. We used the newest neuronavigation techniques (including tractography) and neurophysiological control.
See the video session…

The influence of Functional Neurosurgery on General Neurosurgery
So far, I have given you an outline of the evolution of cerebral cortex surgery.
Now, I would like you to consider the influence General and Functional Neurosurgery have had one on each other and to summarize some important issues.
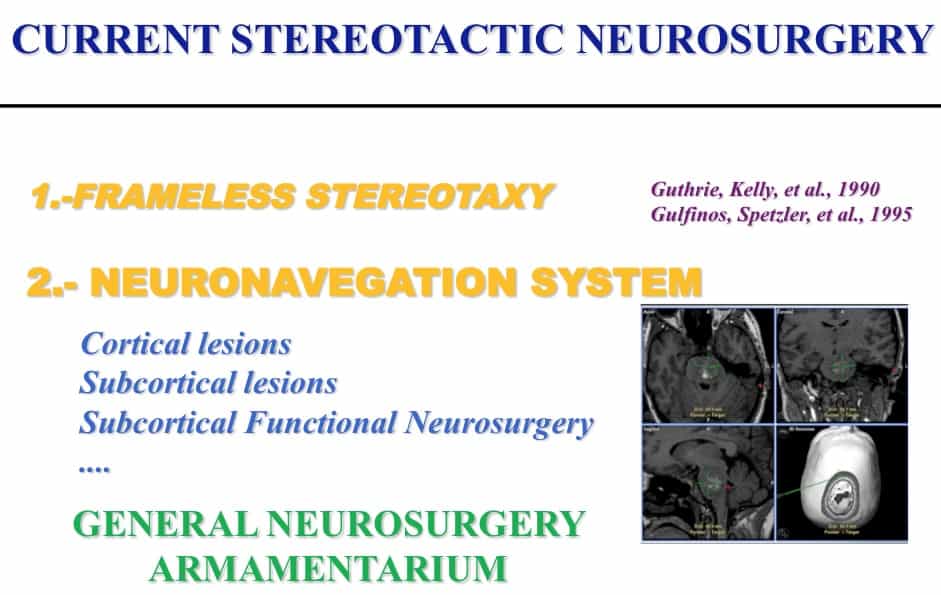
Stereotactic and Functional Neurosurgery
Firstly, the influence of Stereotactic and Functional Neurosurgery on General Neurosurgery.
To begin, I would like to discuss certain basic ideas.
As an example of developments in Stereotactic Neurosurgery that have benefited General Neurosurgery, we can look to the evolution of the frameless stereotaxy concept to the neuronavigation technology, that has become neurosurgical standard practice.
Leksell
Or another is the acceptance of the concept of Radiosurgery. Even to treat pathologies outside the Nervous System.
Fields of functional neurosurgery
In the brunch of Functional Neurosuyrgery, we must emphasize certain fields.
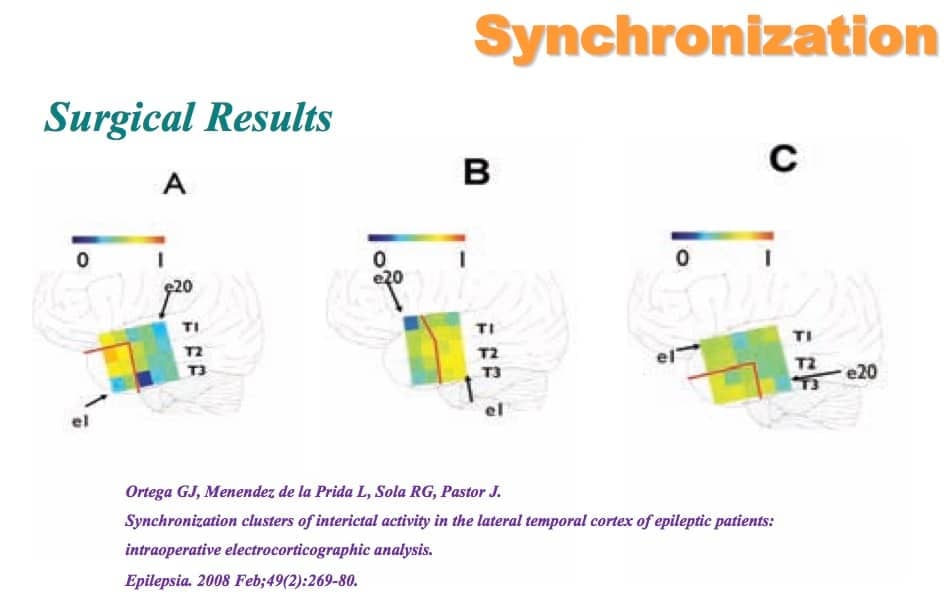
Epilepsy Surgery
One of the most relevant is Epilepsy Surgery, where concepts such as the anatomo-functional map proposed by Talairach and Bancaud have permitted a better design of implantation deep electrodes for Stereoelectroencephalographic recording of epileptic seizures.
Another example is the application of Talairach concept of “normalisation” procedure. It permits us to collect the anatomical and functional results of several patients with similar pathology.
The development of an image integration system like this, adapted to the most modern neuronavigation systems, has permitted us, for example, to implant deep electrodes in the correct epileptogenic area.
Stereoelectroencephalography
And recording of the beginning of the epileptic discharge is possible.
As a routine, we make ECoG recording before the cortical excision of the epileptic focus.
But we are concerned about the capability to obtain in real time anatomical and functional information.
As a first step, we added the microscopic surgical field image to the neuronavigation equipment.
In a second step, we made the effort to design an images integration system, as we have mentioned earlier
Let me show you the surgical view of a mesial temporal lobe epilepsy resection.
We followed Spencer’s surgical technique. We tried to get the resection in bloc of the hippocampus (with the shape of a sea-horse).
See the video session…

Epilepsy surgery research
But epilepsy surgery might be an important research field and we have explored this possibility.
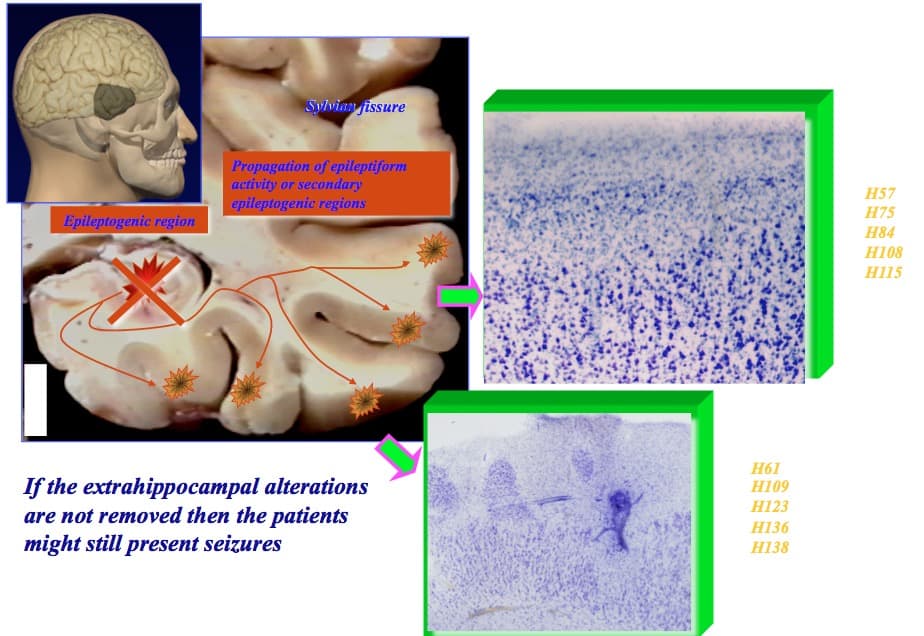
At the beginning, we supported a focal theory.
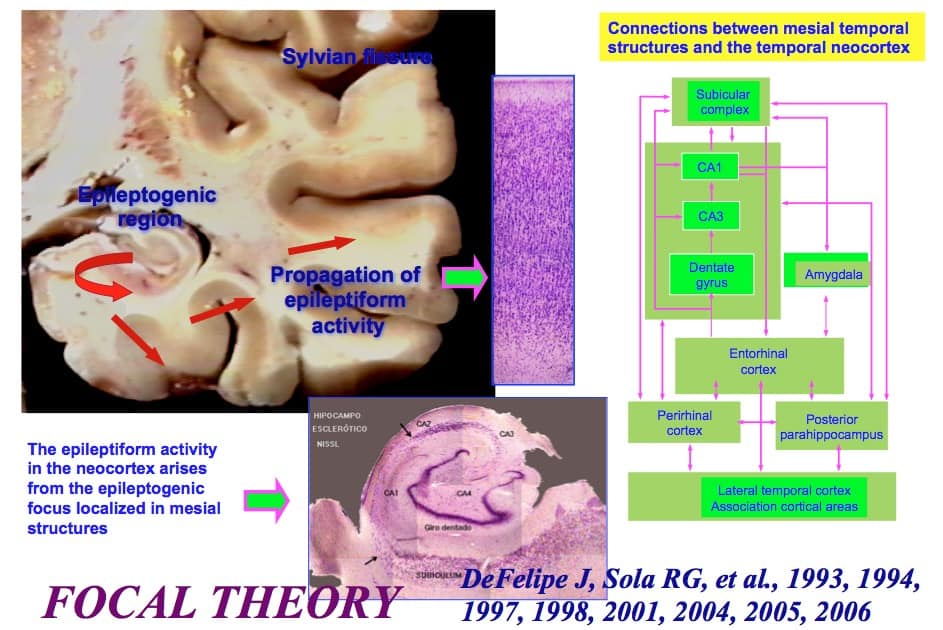
With a principal epileptogenic focus, and its propagation of neocortical areas.
But we observed that if the extrahippocampal alterations are not removed, then the patients might still have seizures.
Susan Spencer
We then evolved to a network conception of epilepsy, as Susan Spencer proposed.
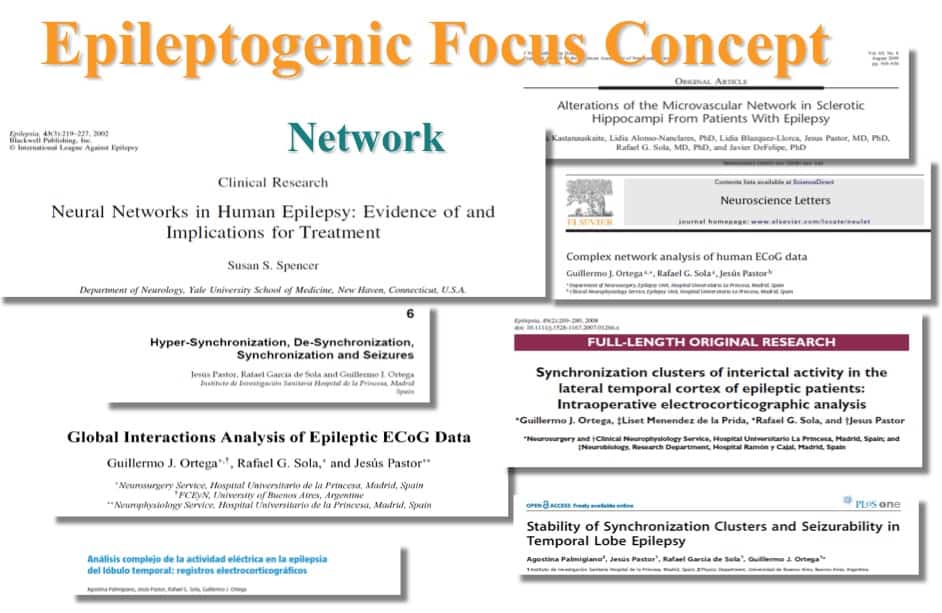
We have described network organization with nodes.
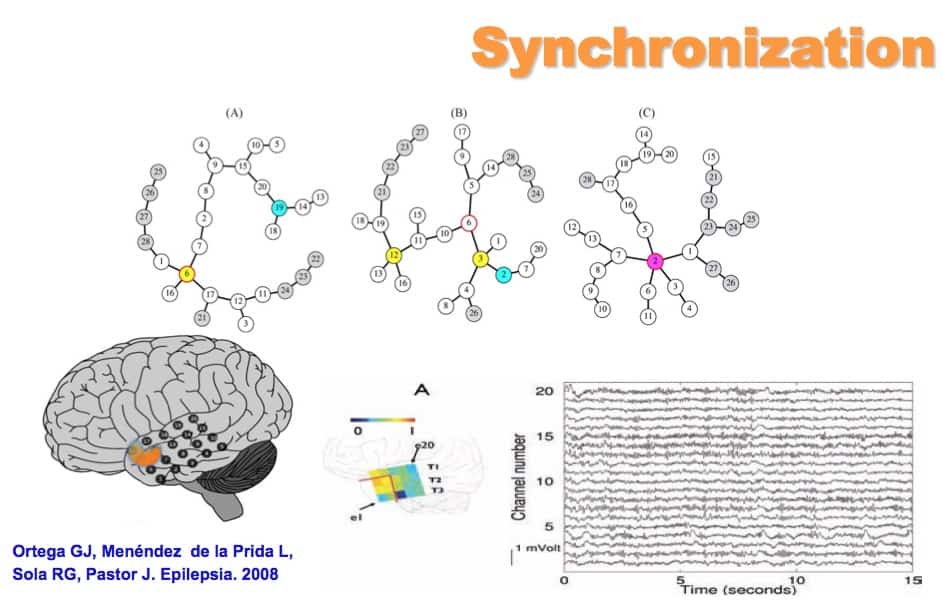
And have observed that surgical results could depend on what neocortical nodes we have removed.
And then, our vision has widened to a more complex concept of the epileptogenic focus. We must accept, for instance, different subtypes of surgical epilepsy.
Neurophysiological monitoring
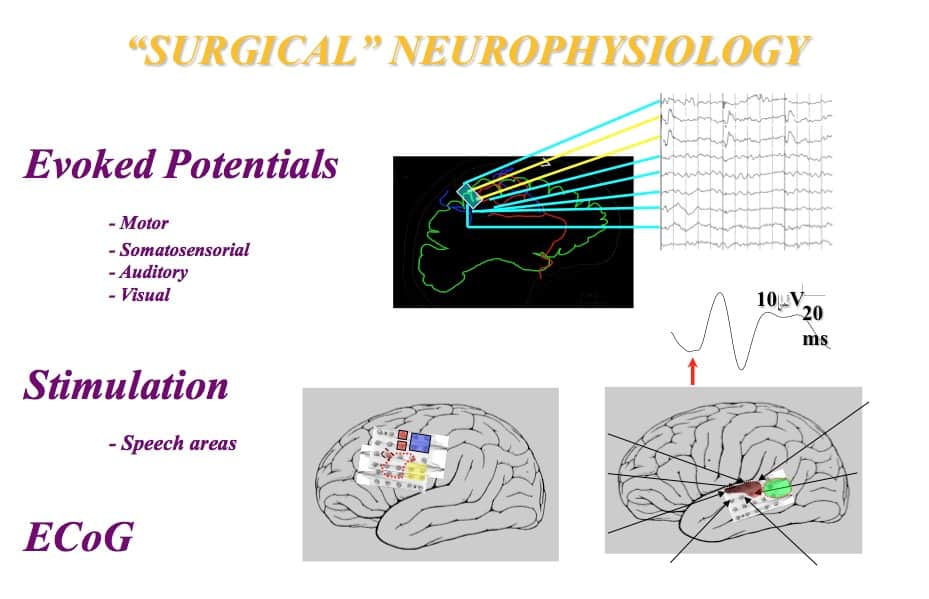
Another relevant field of Functional Neurosurgery is Neurophysiological Monitoring.
It has permitted us to deal with cerebral cortex function in depth.
The intraoperative neurophysiological monitoring, with the useful techniques of evoked potentials, stimulation and recording neuronal activity.
We could make use of this technology, for instance, to control malignant astrocitomas removal guided by Gliolan.
And, in our experience, we have significantly decreased postoperative neurological deficits, achieving high percentages of gross total removal
If you allow me, I will now show you an example of one tumour removal guided by Gliolan and Neurophysiological monitoring.
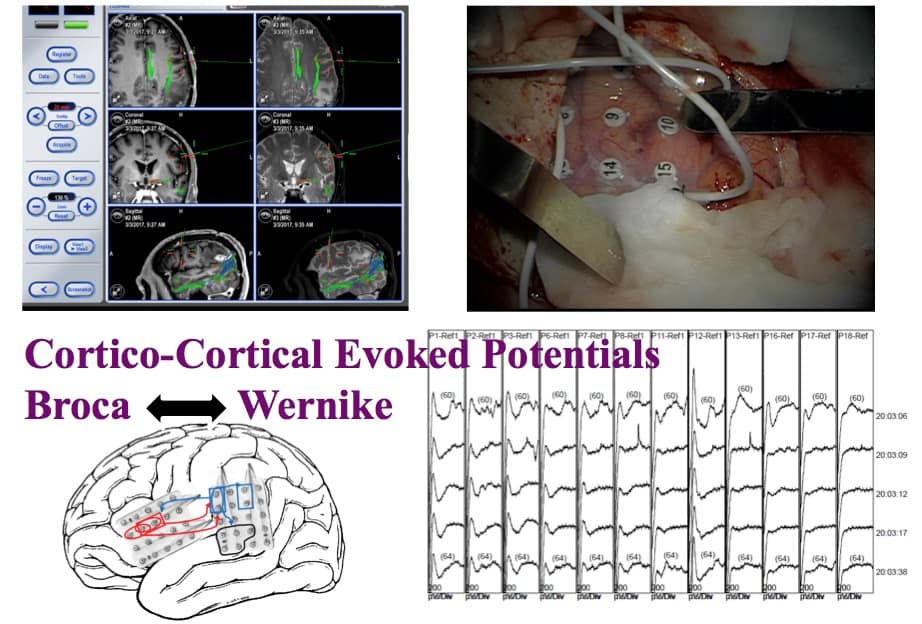
Our new contribution to monitored the speech areas in anaesthetized patients. A continuous registry of the cortico-cortical potentials is made, between the Broca and Wernicke areas.
This would allow, in anesthetized patients, to protect the language areas, as the tumor resection approaches them. And it would even allow the integrity of the tracts involved in the language function.
See the video session…

And the next question must be.
How General Neurosurgery has influenced the development of Stereotactic and Functional Neurosurgery?

Glioma surgery
In a General Neurosurgical Department you have at your disposal all the surgical facilities
Such as Human Resources and the equipment.
This has allowed for a huge development in, for instance, glioma surgery.
Intraoperative neurophysiologial monitoring
With the help of intraoperative neurophysiological monitoring (IONM), we have reached a high level of efficiency.
This is another example of how we have evolved.
See the video session…
Intraoperative neuropsycological monitoring
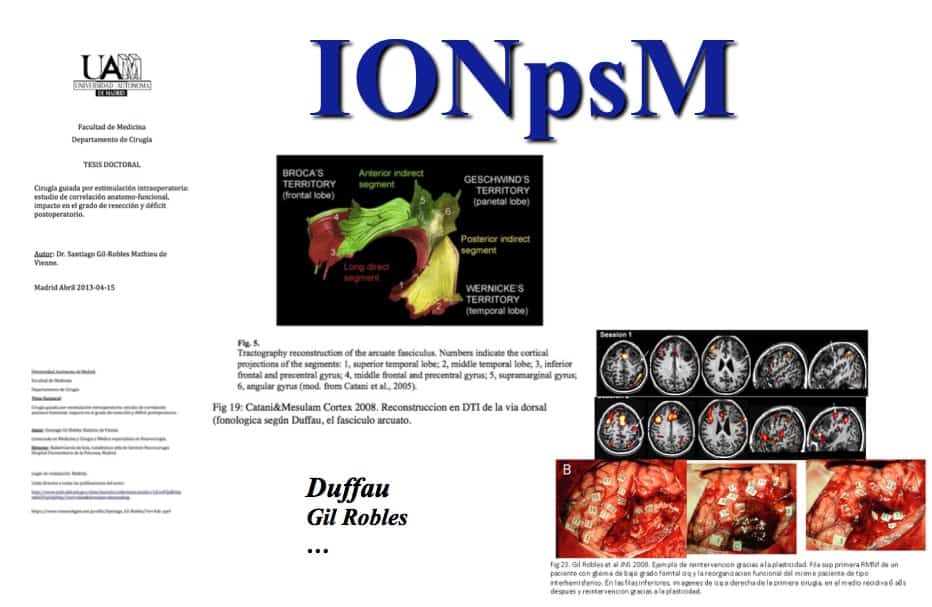
But nowadays authors such as Duffau have promoted neuropsychological assistance for monitoring the patient’ reaction to electrical stimulation.
I had the privilege of directing Gil Robles’s Thesis work on this topic. And we have recognize the importance of this concept in relation to cerebral cortex function.
He is an outstanding disciple of Duffau.
His work was named as the best Thesis by our School of Medicine
Conclusions
To finish, I would like to present several ideas as a kind of conclusions
In big neurosurgical departments, more and more concepts of stereotactic and functional neurosurgery are been accepted in general neurosurgical practice. This means that a certain trend or tendency to fusion exists.
In this context, it is necessary to have everything:
- Firstly, to identify the problem.
- Secondly and very importantly, to design the surgical operation according to the anatomo-functional findings.
- Lastly, to have a correct surgical technique.
To know the problem
– Physiopathology
– Function
– Anatomy
To design the surgical operation
To have a suitable surgical technique
With these premises, we can observe Cerebral Cortex Surgery from the Functional Neurosurgical point of view and divide it into its several components.
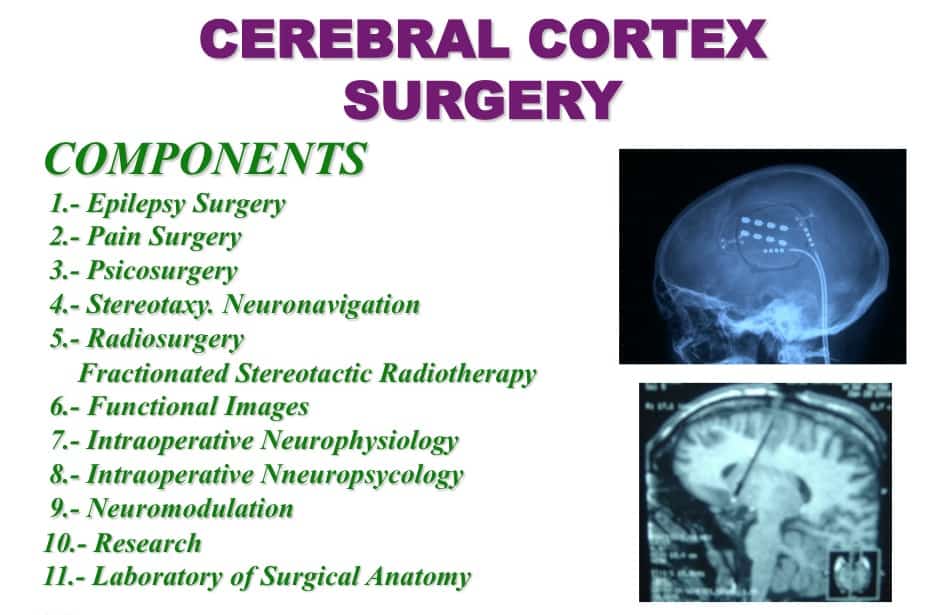
Components
- 1.- Epilepsy Surgery
2.- Pain Surgery
3.- Psicosurgery
4.- Stereotaxy. Neuronavigation
5.- Radiosurgery. Fractionated Stereotactic Radiotherapy
6.- Functional Images
7.- Intraoperative Neurophysiology
8.- Intraoperative Nneuropsycology
9.- Neuromodulation
10.- Research
11.- Laboratory of Surgical Anatomy
But also, we can look at cerebral cortex surgery from the perspective of the general neurosurgery. And to divide it into its three principal branches:
- tumoral,
vascular and
functional surgery.
- I would like to propose that Cerebral Cortex Surgery be considered a sub-speciality, based on the anatomical location (as, for example, the skull base surgery).
- Secondly, I would like to propose the inclusion of Epilepsy Surgery and the other functional surgical fields in this sub-speciality.
- My final proposal is that, as Cerebral Cortex Surgery is closer to Stereotactic Functional Neurosurgery, the former might be led by the latter and scientific societies as SENFE.
Thank you.