Harmony in the neurosurgical operating room
Director de la Cátedra UAM de “Innovación en Neurocirugía”
Facultad de Medicina. Universidad Autónoma de Madrid (UAM)
1.- Distribución adecuada y estable del personal que está implicado en una intervención quirúrgica.
2.- Distribución adecuada de toda la tecnología, con el propósito de que sea manejada de la forma más eficiente posible.
3.- Que el quirófano se adapte con mínimos cambios a cirugías tan diferentes como los abordajes cráneo-encefálicos, raqui-medulares, endoscópicos o de Neurocirugía Funcional
4.- Que al final se consiga:
a) Mantener la atención y, por consiguiente, la colaboración de todo el equipo quirúrgico en todo momento de las acciones que se están llevando a cabo. Disminuye extraordinariamente el nivel de sorpresa y de riesgos imprevistos.
b) Conseguir un ambiente de armonía y seguridad quirúrgica.
Harmony in the Neurosurgical Operating Room
Neurosurgical Operating Room: Harmony between human team and technological advances
Director of the UAM Department of «Innovation in Neurosurgery».
Faculty of Medicine. Universidad Autónoma de Madrid (UAM)
The need for a conception of the Neurosurgery Operating Room with several objectives arises:
1.- Adequate and stable distribution of the personnel involved in a surgical intervention.
2.- Adequate distribution of all the technology, with the purpose of managing it as efficiently as possible.
That the operating room adapts with minimal changes to surgeries as different as cranio-encephalic, spinal-medullary, endoscopic or functional neurosurgery approaches.
4.- That at the end it is achieved:
- (a) Maintain the attention and, consequently, the collaboration of the entire surgical team at all times of the actions being carried out. It reduces extraordinarily the level of surprise and unforeseen risks.
b) To achieve an atmosphere of harmony and surgical safety.
Neurosurgical operating room harmony between human team and technological advances.
INTRODUCTION.
Hospital
MISSION.- Adequate means to deal with situations of extreme gravity
STRUCTURES that stand out:
A.- The Emergency Services.
B.- Critical Care Units (ICU, REA, Coronary, Ictus …).
C.- Operating Rooms.
Technologically very demanding.
Enough space?
Lavishness in other hospital structures?
Operating rooms
Its existence is impossible without the hospital environment
Evolution in the design team:
1º.- It was the surgeons themselves.
2º.- Very complex technical demands.
Currently, many people are involved who do not «step on»
the operating rooms.
3º.- Surgeons are hardly consulted.
Current results:
– Reduced spaces. Operating rooms and annexed rooms.
– Restricted, Corseted.
– There is no vision of the future, nor of the technological development that is taking place.
Operating rooms conception
1.- Operating rooms for the development of a very specific technique.
- – It is usually proposed by certain surgeons.
– «Smart» operating rooms are made with lots of «dumb, passive» screens.
– If the techniques change or the surgeon stops working,the operating room becomes obsolete.
– In reality, its life is very limited and the cost is very high
2.- Wide surgical spaces, open to any surgical specialty.
- – Minimum: 70-80 m2
– All equipment has wheels.
The operating room can be emptied, cleaned
and used by another specialty.
– Technologically well equipped
(security systems, gases, electrical networks, internet, WiFi , screens-images, networks…)
– Improves efficiency and competitiveness among surgical teams.
SURGICAL TECHNOLOGY
A.- Everyone talks about lasers, robots, neuronavigation, 3D vision…
B.- Large hospital companies assume very important expenses in a certain technology, to give an imprint of confidence.
C.-. Sometimes there is no relationship between the dynamics of these complex technologies (Radiotherapy, Imaging …) and the technological reality of their operating rooms themselves.
D.- Obscure marketing goals, leveraging the acquisition of flashy technology?
Development Periods
I.- Years 40-50 to 80-90
Technological advances proposed by the surgeons themselves:
Cushing, Penfield, Talairach, Leksell, Yasargil, Malis …
Coagulation, Microscope, Radiosurgery, Stereotaxy….
II.- Years 70-90
Technological advances parallel to the neurosurgical effort :
Great development and design in: Images, navigation, radiotherapy …
III.- XXI century
Independence of engineering teams developing new technologies
XXI century
1.- The surgeons are being invaded by new ideas.
– Very attractive
– Adaptable to their surgical reality?
2.- Examples:
– New concepts in Neuronavigation-Images integration
– Robotic-neuronavigated MICRO-EXOSCOPE.
3.- These new developments require significant training
– Limitations?
– Immaturity?
– Should we force the surgical attitude?
Less urgency and economic pressures could be needed.
NEUROSURGERY OPERATING ROOM
Preliminary considerations
1.- Neurosurgeons have high technical training:
– Independent
– They are continuously developing new approaches
– They must be provided with a comfortable habitat intellectually and physically.
2.- The nursing staff is usually unstable
– Sometimes with a low level of neurosurgical knowledge
3.- Other technicians (Radiology, Companies …)
– Sometimes with deficits of knowledge-interest
4.- Other professionals: Anesthesia, Neurophysiology, Psychology, Neurology….
FIRST: To design fixed spaces for staff:
– Anesthesia
– Nursing
– Technicians
– Neurophysiology …
SECOND: Regardless of whether a neurosurgical approach is carried out at the cranio-encephalic or spinal cord level.
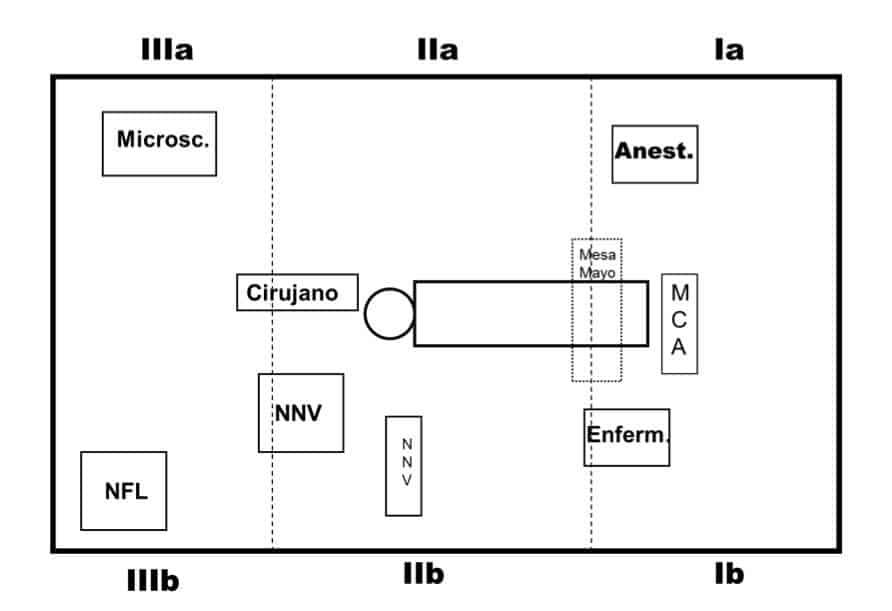
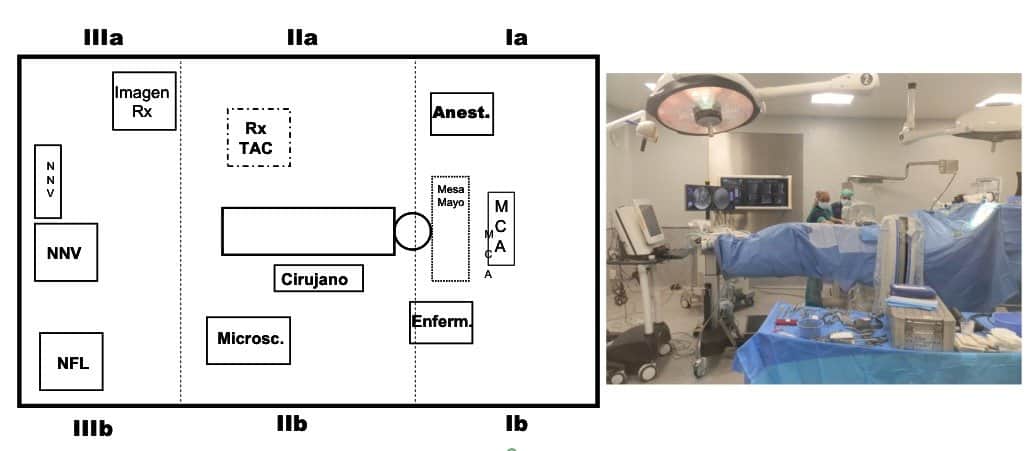
1st.- Distribution of surgical space
The operating room area is divided into 3 spaces:
I.- For Anesthesia (Ia) and Nursing (Ib)
– Anesthesia team …
– Basic equipment (motors, coagulation, suckers…)
II.- Surgical area of the patient
– Surgical field
– Surgeons and assistants
– Neuronavigation device (it changes the side, according to the right-left approach)
III.- Complementary area:
– Microscope
– Neurophysiology
– Other equipment (?)
In Spine surgery, the same spaces can be maintained:
I.- For Anesthesia (Ia) and Nursing (Ib)
– Anesthesia team …
– Basic equipment (motors, coagulation, aspiration …)
II.- Surgical area of the patient
– Surgical field
– Surgeons and assistants
– CT-Scan-NNV
– Microscope, Endoscope…
III.- Complementary area:
– Neuronavigation
– CT-Scan screen
– Neurophysiology
– Other equipment (…)
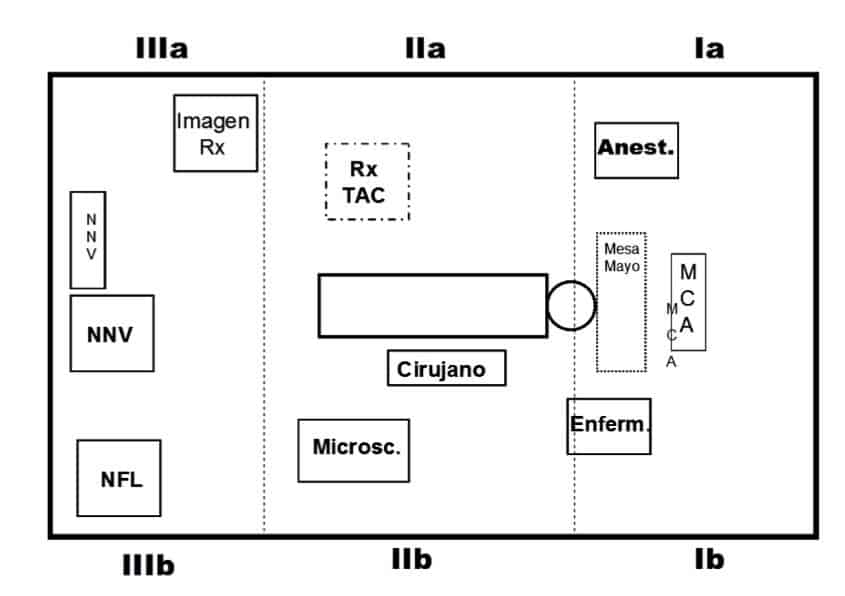
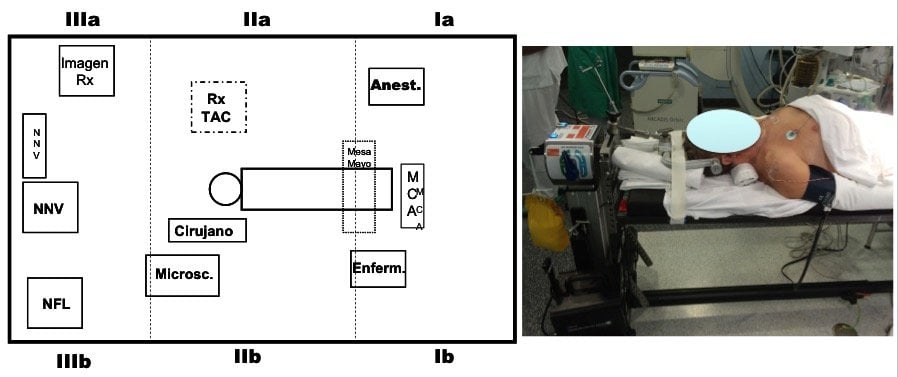
2nd.- DISTRIBUTION OF SURGICAL SPACE
Have very different surgical approaches in mind
Sometimes it is preferable not to change positions, although the right-handed surgeon may have to be a bit more uncomfortable.

Only the Rx equipment moves to the right of the patient.

Sometimes it is preferable not to change positions, although the right-handed surgeon may have to be a bit more
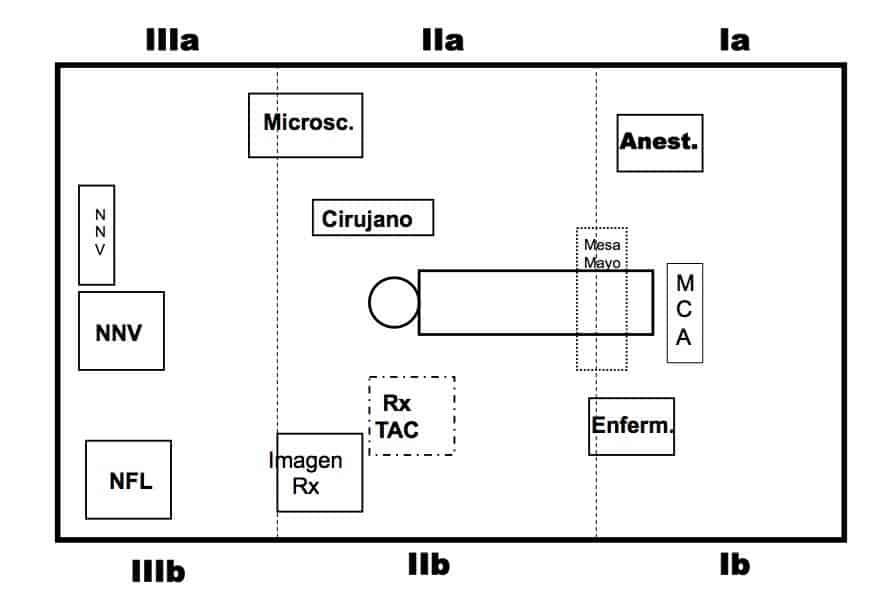
RESULT OF HARMONIZATION
Same assignment for cranial and spine surgery

Example of distribution in cranial surgery, maintaining the same spaces.
Approach from the left side. The Neuronavigator is on the right side.

Example of distribution in cranial surgery, maintaining the same spaces.Approach from the right side. The Neuronavigator is on the left side.

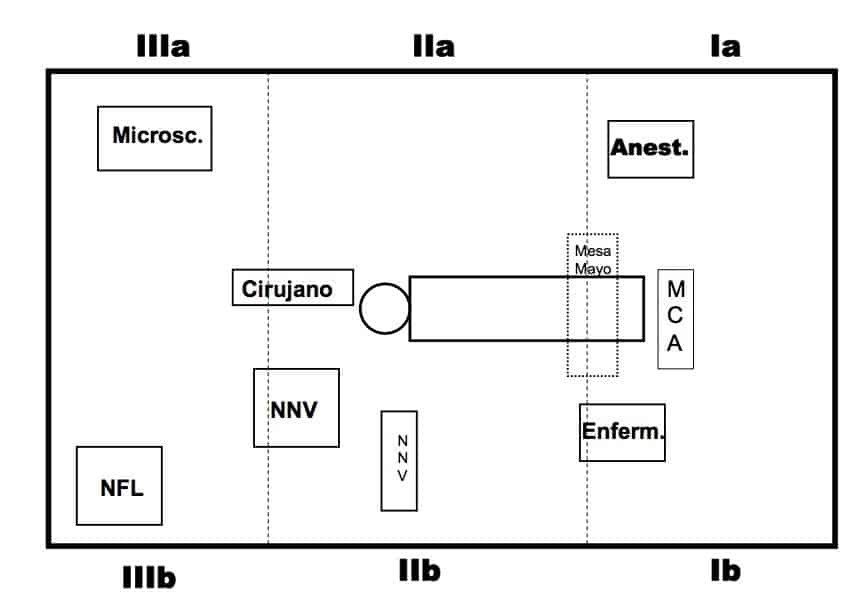
Surgical approach to the posterior part of the cervical spine.
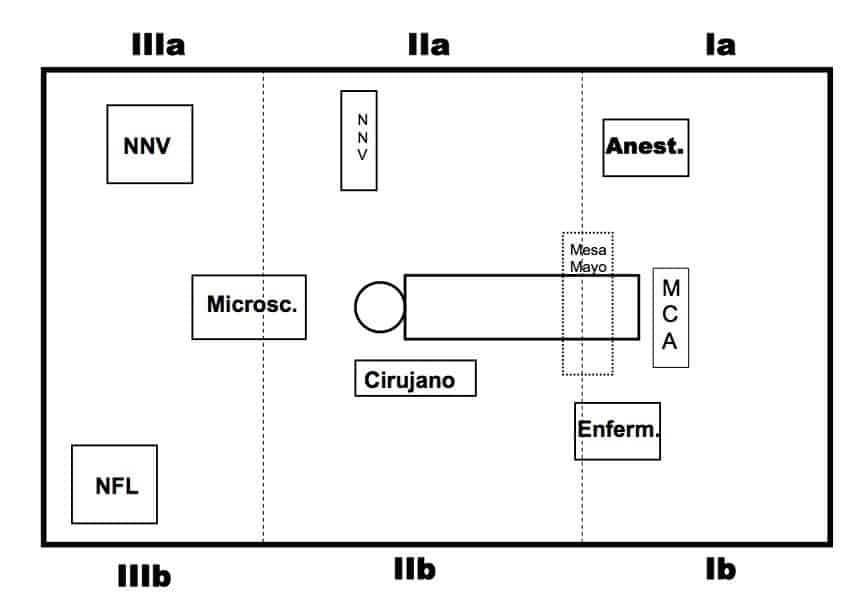
Example of distribution in anterior cervical surgery, maintaining the same spaces.
Approach from the right side to the anterior neck.
The patient is positioned on a Jackson Table, with cervical traction and allowing intraoperative CT and Neuronavigator control.
Example of distribution in posterior cervico-thoracic surgery,
maintaining the same spaces.
Approach from the right side to the posterior neck.
The patient is positioned on a Jackson Table, with cervical traction and allowing intraoperative CT and Neuronavigator control.
The patient is positioned on a Jackson Table, with cervical traction and allowing intraoperative CT and Neuronavigator control.
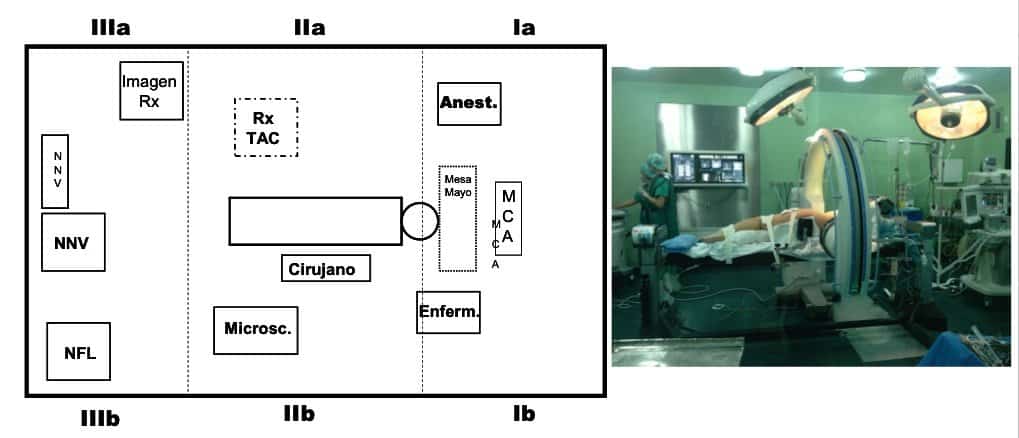
Example of distribution in thoracic surgery, keeping the same spaces.
Image of an operating room at the Hospital de La Princesa. Madrid
Approach from the left side to the thorax.
The patient is positioned on a Jackson Table and allowing intraoperative CT scanning and Neuronavigator control.
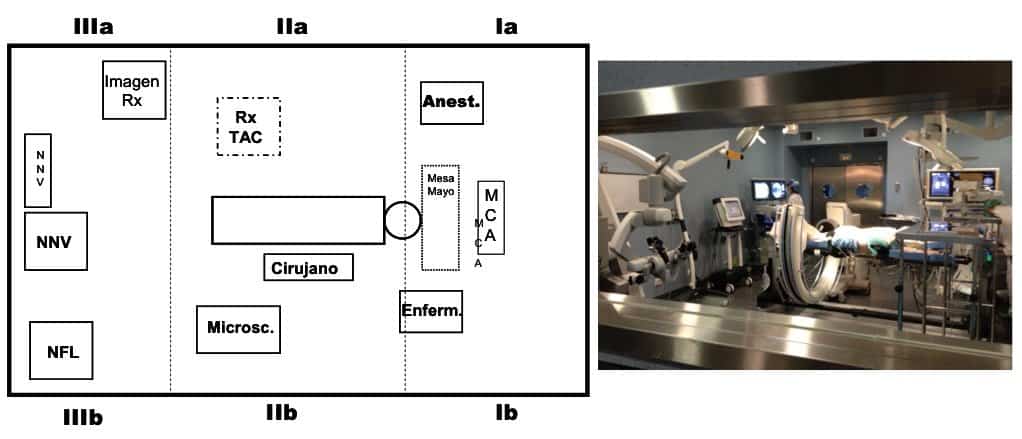
Example of distribution in lumbar surgery, maintaining the same spaces.
Posterior approach.
The patient is placed on a Jackson Table, allowing for intraoperative CT and Neuronavigator control.
Operating room of Hospital del Rosario. Madrid.
NNV reference “stars” in the iliac crest.
Example of distribution in thoracic spine surgery, maintaining the same spaces.
Posterior approach.
The patient is positioned on a Jackson Table, allowing intraoperative CT scanning and Neuronavigator control.
Image of an operating room at the Hospital de La Princesa. Madrid.
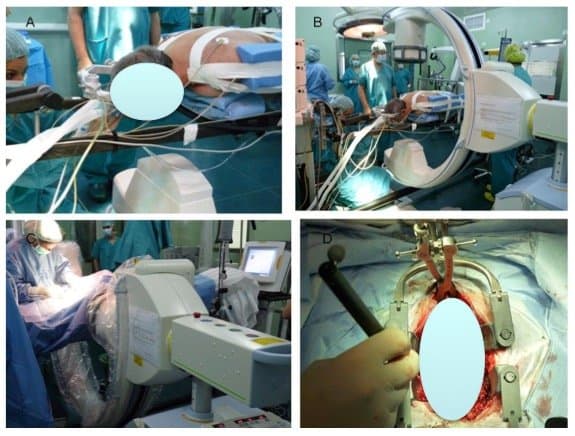
NEW TECHNOLOGICAL ADVANCES
Minimally invasive surgery

Lumbar Microhemilaminectomy + Pedicular Fixation. MIS approach. Microscope, 3D-NNV, x-Ray….
Surgical intervention recorded on an image integration system.
Simultaneous surgical movements are visible on the different screens of the operating room: Anesthesia, Ambient Camera, Microscope, Neuronavigator, CT, Planner…
First of all, a reference system for the neuronavigator, fixed on the iliac crest, is placed.
A CT scan is then performed and the data is passed to the neuronavigator.
Under the control of the neuronavigator, a special retractor is first placed to reach the hemilamina and perform microsurgical decompression of the trapped nerve root and widen the space in the stenotic area. The Neuronavigator guides the surgeon in these maneuvers at all times.
In a second stage, also with minimally invasive techniques, pedicle screws are placed.
The punctures, taps and screwdriver are calibrated with the Neuronavigator.
Finally, a new intraoperative CT scan confirms the correct position of the pedicle screws.
IMAGE INTEGRATION ROBOTIZATION
Go to our website: neurorgs.net

FUTURE
Smart Operating Room
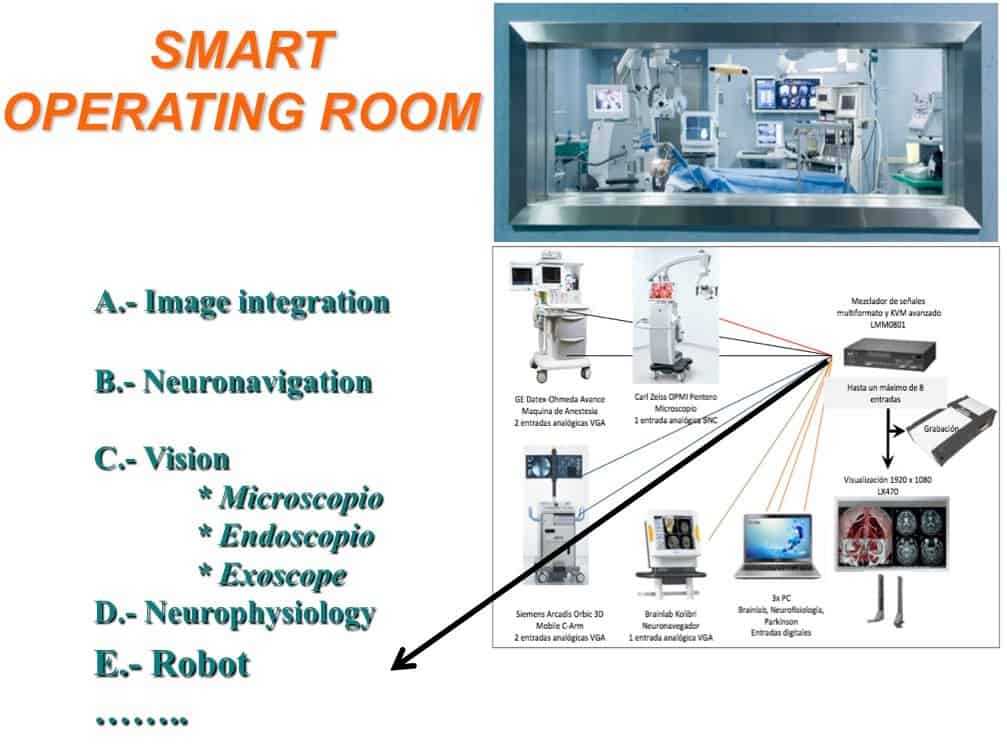
A.- Image integration
B.- Neuronavigation
C.- Vision
* Microscopio
* Endoscopio
* Exoscope
D.- Neurophysiology
E.- Robot
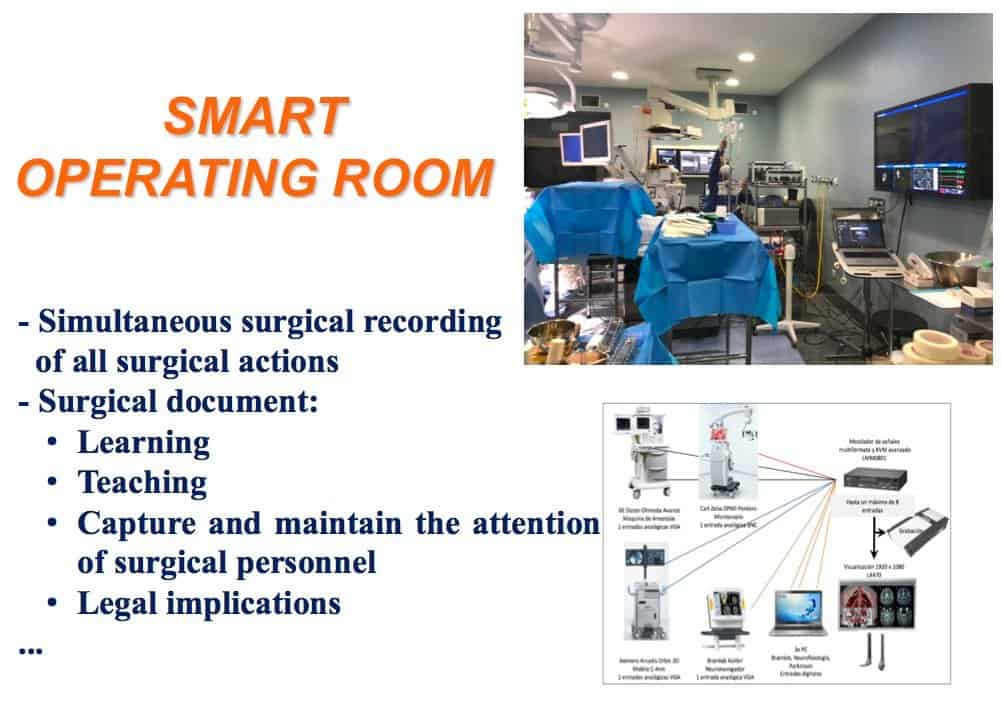
– Simultaneous surgical recording
of all surgical actions
– Surgical document:
- Learning
Teaching
Capture and maintain the attention of surgical personnel
Legal implications
CONCLUSIONS
Acquire knowledge and skill with new technologies
The best Operating Room location must be searched
Keep in mind that the technological development process has just begun
Set priorities
Operating room staff

A.- Surgeon and surgical assistants
B.- Anesthesia
C.- Neurophysiology
D.- Nursing
– Scrub nurse
– Auxiliary staff
E.- Image
– C-arm
– CT-Scan
– Neuronavigation
– Ultrasound
F.- Research team
G.- Staff, Residents, Students and Visitors
EQUIPMENT
A.- Surgical table
– Cranioencephalic surgery
– Jackson spine table
B.- Microscope
– Gliolan
– Indocyanine Green
C.- Stereotaxic Guide
D.- Endoscopy
E.- Ultrasonic Aspirator
I.- Bipolar coagulation, Motor, Aspiration …
J.- ROBOT
K.- EXOSCOPE
1.-Neuronavigation device
– Cranial
– Spine
2.- Intraoperative Neurophysiological Monitoring
3.- x-Ray Equipment
– C-Arm
– 3D arm
4.- Ultrasounds
5.- Flowmeter
6.- Work station
7.- Digital Box
Exoscope

AIM:
- Training. Experience
Teaching.
Wide the surgical capacity
Improve approaches: (spine surgery)
Keep the attention on this new development
New equipment: 3d vision at the microscope


ADVANTAGES:
– Experience in 3D vision
– Involve surgical staff throughout the procedure
– Teaching
– ….
Objectives:
- Improve 3D vision experience.
Involve the staff’s interest in the procedure being performed.
The staff understands the surgical intervention and collaborates much more closely.
Teaching
….
Teaching
Improve surgical capacity in some processes
Improve surgical approaches
Maintain focus on current technological development
Robot-endoscope ROSA®

ADVANTAGES:
– Solid and secure holder
– Smooth and controlled handling
– Improve surgical comfortableness
– 3/4 hands surgery
– Neuronavigation
A.- Surgeon and Assistants
B.- Anesthesia
C.- Neurophysiology
D.- Nursing
– Instrumentalist
– Surgeon
– Auxiliary Staff
E.- Imaging
– Amplifier
– CT
– Neuronavigator
– Ultrasound
F.- Staff specialized in implants
G.- Staff, Residents, Students and Visitors
SURGICAL STAGES in a surgical professional career
Experience Curve vs Learning Curve
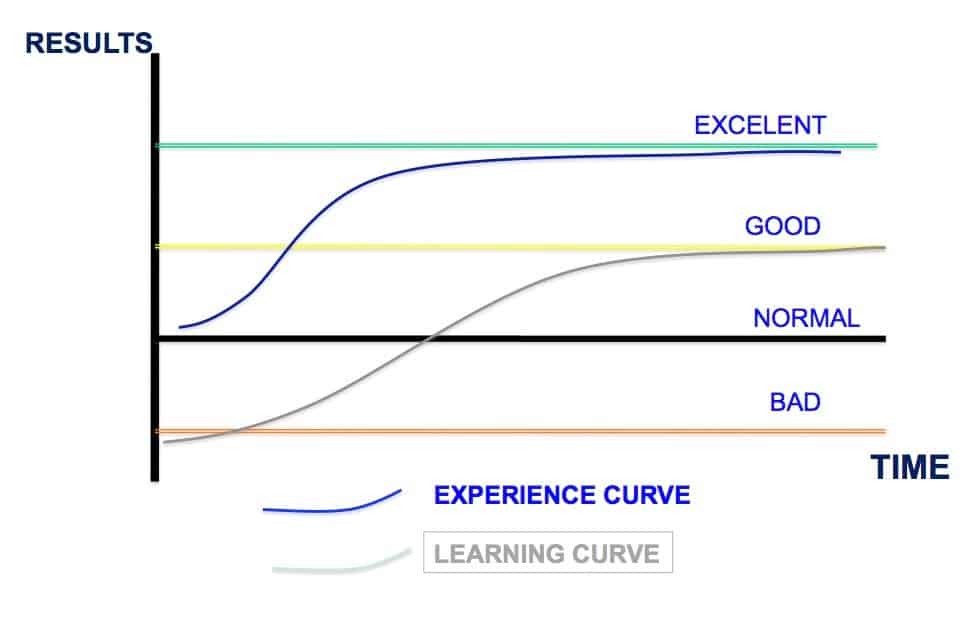
The Learning Curve could start the activity below standards, until the surgeon achieves experience and reasonable results.
But, by publishing such results, it could ignore the first phase…
The Experience Curve means that the surgeon is already an expert. And he starts from a zone of normal performance level.
With experience, he reaches much better results.
He publishes his results from the beginning.
Learning Curve
Proper term?
Surgeons begin to learn.
They get a good level.
They publish, forgetting the beginner failures…
THE PRICE OF THE INITIAL SURGICAL FAILURES COULD BE HIGH
Experience Curve
The surgeon already has experience in similar fields
He begins to develop the technique,
from a medium-high level of execution
He gains experience fast and achieves excellence
It is possible to publish results, including the first cases
Neurosurgical Anatomy Labs

In collaboration with UAM Chair “Innovation in Neurosurgery”
The best way to learn is to visit and work in the Surgical Anatomy Laboratories (Cadaver Surgery).
And then, move on to the real operating room.
Vision of our Laboratory in the Department of Anatomy of the Faculty of Medicine of the UAM.
SURGICAL STAGES in a surgical professional career
Like the music performers (?)
1st.- Fine surgical approach, even if it’s slow.
2nd.- Good. More and more agile execution.
3rd.- Aesthetically correct. It could be seem “simple” to the “inexperience” observers.
4th.- Surgical procedure likes, attracts its attainment.
5th.- Mastering the pathology, the surgical performance.
HARMONY IN THE NEUROSURGERY Operating Room

In the end, the serene, calm and harmonious environment of the operating room is very important.
Vision of a joint ENT and Neurosurgery operation (endonasal endoscopic approach, with Robot).
HARMONY IN THE NEUROSURGERY Operating Room

In the end, the serene, calm, harmonious environment of the operating room is very important.
Vision of a surgical intervention, in the same operating room (Hospital del Rosario), to implant an electrode in the subthalamic nucleus. For treatment with deep brain stimulation in a patient with Parkinson’s disease.