Role of intraoperative neurophysiological monitoring during fluorescence-guided resection surgery
Papel de la monitorización neurofisiológica intraoperatoria durante la cirugía de resección guiada por fluorescencia
El Dr. Rafael García de Sola y su equipo analizan en este artículo como la monitorización neurofisiológica intraoperatoria (IONM) puede ser útil durante la cirugía para maximizar la resección tumoral, mientras tanto ayuda a evitar déficits neurológicos y, por tanto, a mejorar la calidad de vida de estos pacientes.
Rafael García de Sola
Director de la Cátedra UAM “Innovación en Neurocirugía”
Jefe del Servicio de Neurocirugía
Hospital Ntra. Sra. del Rosario
Madrid
Jesús Pastor, Lorena Vega-Zelaya, Paloma Pulido, Oscar Garnés-Camarena, Angela Abreu and Rafael G. Sola
Lorena Vega-Zelaya and Paloma Pulido contributed equally to this work.
J. Pastor (*) : L. Vega-Zelaya : O. Garnés-Camarena : A. Abreu Clinical Neurophysiology, Hospital Universitario de La Princesa, C/Diego de León 62, Madrid 28006, Spain e-mail: jpastor.hlpr@salud.madrid.org
P. Pulido : R. G. Sola
Neurosurgery, Epilepsy Unit, Hospital Universitario de La Princesa, Madrid, Spain
J. Pastor : P. Pulido : R. G. Sola
Unidad de Neurocirugía, Nuestra Señora del Rosario, Madrid, Spain
R. G. Sola
Faculty of Medicine, UAM, Madrid, Spain
Acta Neurochirurgica. The European Journal of Neurosurgery ISSN 0001-6268
Acta Neurochir
DOI 10.1007/s00701-013-1864-0
Received: 28 June 2013 / Accepted: 25 August 2013
Copyright: Springer-Verlag Wien 2013
Abstract
Background
Fluorescence-guided resection (FGR) using 5-aminolevulinic acid (5-ALA) exhibits a potential risk of permanent neurological deficits that can be minimized using intraoperative neurophysiological monitoring (IONM). We assessed the role of IONM in FGR surgery in patients harboring tumors in or near eloquent areas.
Methods
IONM and FGR surgeries were performed on 34 patients (49.8±2.4 years) harbored malignant primary gliomas near eloquent cortical areas or semioval center. Different combinations of neurophysiological techniques were used depending on each patient.
Results
Gross total resection (GTR) was achieved in 66.7 % of the patients, mean 90.4±3.7 % without neurological deficits. Resection in four patients was stopped by the occurrence of severe warning criteria despite the presence of fluorescence. Hemispheric transcranial electrical stimulation was safe and confident even in cortical surgery. Notably, a significant percentage of patients exhibited clinical improvement after the surgery. One week after surgery, only one patient worsened, and seven patients improved. At 3 months, 27.8 % of the patients improved, and the other patients maintained a similar status to their pre-surgery condition. Warning common criteria (amplitude reduction and/or latency increase) appeared in 68.2 and 50.0 % of patients during cortical or semioval surgery, respectively, with neither a false-negative nor a false-positive clinical outcome. Although 5-ALA exhibits phototoxicity, VEP did not induce any secondary effects in the visual system, including eyelids.
Conclusions
IONM can be helpful during surgery to maximize the tumor resection, meanwhile help to avoid neurological deficits and, therefore, to improve the quality of life of these patients.
Keywords
: 5-aminolevulenic acid. Direct cortical stimulation. High-grade gliomas. Motor-evoked potentials. Somatosensory-evoked potentials. Visual-evoked potentials

INTRODUCTION
Intraoperative neurophysiological monitoring (IONM) is a powerful technique that provides increased functional knowledge during surgical operation, which results in the safer removal of a radical tumor [9, 16]. These aspects are particularly relevant in patients suffering from high-grade gliomas, where survival is directly related to the degree of tumor removal [23, 24].
Recently, 5-aminolevulinic acid (5-ALA) has been used in neurosurgery to resection high-grade gliomas [22]. 5-ALA induced protoporphyrin IX (PpIX) is used in the fluorescence-guided resection (FGR) of malignant diseases. Administered in an oral form, 5-ALA penetrates the tissue in a suboptimal manner. Accumulation of PpIX is elevated in many malignant tissues, several tissue abnormalities, and in mucosa [8]. This accumulation can be visualized by irradiating the patient with a blue light (wavelength of 400 nm). It has been shown that radical resection is greater when FGR is used [23] and that progression-free survival is enhanced in patients who are operated on with 5-ALA [22].
However, in patients whose tumors are located near the inner capsule (IC) or thalamocortical fibers (ThCF) (e.g., either in the somatosensory or visual systems), it is extremely important to identify relevant tracts to preserve good functionality in the patient [5]. Thus, resections performed using a tool such as 5-ALA carry a risk of temporary or permanent impairment in neurological function [3, 26]. Recently, tractography by diffusion tensor imaging (DTI) and intraoperative magnetic resonance imaging (MRI) have proven to be useful in IC or ThCF identification [1, 28]. However, dynamic changes during surgery (loss of cerebrospinal fluid, low-grade brain edemas) and the lack of reliability in the identification of small or functional tracts pose potential risks [6, 15]. Thus, it is extremely important to be confident during the entire surgery regarding the physiological state of the patient’s motor and sensory systems, which may be provided by IONM.
Several studies have shown the usefulness of 5-ALA in the resection of malignant brain tumors [5, 10, 22, 24, 25] however, a radical resection always carries the danger of causing neurological deficits, particularly, during the removal of tumors in or near eloquent areas of the brain. However, enhancing the ability to maintain or even improve the quality of life in these patients is equally, if not more, important, because of the patient’s very limited life expectancy.
We designed a prospective study to evaluate the utility and limitations of combining FGR and IONM in the surgery of primary malignant brain tumors in or near eloquent cortical areas and subcortical tracts, particularly in relation to the short-term functional outcome after surgery and with a specific focus on the role of intraoperative neurophysiology.
AIMS AND LIMITS OF CORTICAL SURGERY
From a surgical point of view, the cortex can be divided into two classes: i) the primary or eloquent cortex, which cannot be removed or injured because a permanent neurological deficit would appear, and ii) the non-eloquent cortex (secondary and association areas), regions whose function can be supplied by other areas or by means of plasticity.
Cortical surgery, especially neuro-oncology, is a great challenge for neurosurgeons from two perspectives: first, in some types of tumours, gross total resection (GTR) is the best predictor of outcome in terms of life expectancy, mostly for malignant gliomas [6,7]; second, a dominant goal of every surgery is to avoid new iatrogenic lesions. The relative weight of each of these principles can be changed based on individual considerations of the type of tumour, the structures affected, the life expectancy and even the social considerations of each patient. These features are particularly relevant to patients suffering from high grade gliomas, for whom survival is directly related to the degree of tumour removal. Therefore, to maintain an adequate quality of life, the primary goal of surgery is to achieve GTR without compromising neurological function.
These considerations are extremely relevant at the time of making decisions during the surgery, as sometimes it is more important to remove more tumour, knowing that it is placed in a non-eloquent cortex, thus allowing longer survival without neurological deficits (although some transitory deficit can usually be observed) and preserving non-primary functions at the expense of leaving greater tumour volume, which will ultimately shorten the life expectancy.
With these options in mind, our goals during cortical/subcortical surgeries are two: first, to positively identify the eloquent regions and second, to preserve those structures (cortices and tracts coming from and going to) whose injury would induce permanent deficits. Our approach, therefore, is to maximize tumour resection until a primary/eloquent structure is reached.
Methods
Patients
A prospective study performed between November 2009 and March 2012 included a total of 34 consecutive patients (19 males and 15 females) with a mean age of 49.8±2.4 years, harboring malignant primary brain tumors in or near eloquent areas. Two male patients were operated on twice due to tumor recurrence. This study was approved by the Ethical Committee of the Hospital de la Princesa and Clínica Nuestra Señora del Rosario. Informed consent was obtained from all of the patients. Only patients with a Karnofsky Performance Scale score of at least 70 % underwent a fluorescence-guided tumor resection and were included in this study. Neurological examinations were performed in the first week prior to the surgery. Follow-up examinations were performed on the first postoperative day, first week, and third month following surgery. The clinical assessment included the motor status (graded scale: 0=no contraction, 1=flicker or trace contraction, 2=movement with gravity eliminated, 3= movement against gravity, 4=movement against resistance, 5=normal strength), sensory status and visual field evaluation by confrontation.
Magnetic resonance imaging
Preoperative and postoperative imaging included T1-weighted 3D magnetization-prepared rapid gradient echo (MPRAGE) magnetic resonance imaging (MRI) with and without contrast enhancement and T2-weighted sequences to visualize the edema. Diffusion tensor and functional MRI were performed in some patients to visualize the functional cortical areas and cerebral fiber tracts, respectively.
The extent of the tumor resection was determined on the basis of manual segmentation of the tumor outline across all of the sections on an MRI scan. Contrast MRI was performed 72 h after the surgery and compared with the preoperative study. In the tumors that showed contrast enhancement, only the volume bound by the contrast enhancement was segmented. In other cases, the entire area of increased intensity on the T2-weighted images was segmented. If the tumor consisted of enhanced and non-enhanced areas, then both areas were measured [28]. A gross-total resection (GTR) was defined as a reduction of >98 % in the tumor volume on the basis of volumetric measurements.
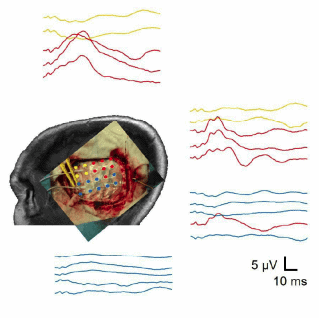
Intraoperative neurophysiological monitoring
IONM was performed (32-channel Elite, Cadwell, Kennewick, Washington, USA) as follows, using different techniques depending on the tumor location.
Electrocorticography (ECoG) was systematically performed before electrical stimulation of the cortex, via a grid of 4×5 electrodes (Ad-Tech, Racine, Wisconsin, USA) of 1.3 mm in diameter and 1 cm center-to-center. The bandwidth was 1.5–1,000 Hz with the notch on. We have used the definitions of after-discharge and irritative zone as usual [17]. We performed during all the ECoG recording a spectral analysis using a fast Fourier transform (FFT) with windows of 8 s. These results are shown as density spectral array (DSA) for a frequency range from 1 to 50 Hz. We defined the lesional cortex as the regions where the DSA showed a clear relative reduction in all the analyzed frequencies.
Direct cortical stimulation (DCS) was performed in two different ways: (1) using pairs of grid electrodes (the cathode was placed as far from the stimulation area as possible), or (2) sometimes, a monopolar probe (anode stimulation, φ=1 mm) was used with a cathode placed on the scalp. In both cases, the same DCS paradigm for was used: constant-current trains of 4–6 pulses at 500 Hz and a pulse width of 150 s, with intensities between 4–30 mA, in steps of 2 mA, starting from 4 mA. Subcortical stimulation (ScS) was performed using the same monopolar probe and same paradigm, with the exception that a cathode current was used to stimulate and the pulse duration was 100 μs. Motor-evoked potentials (MEPs) were recorded through a pair of subdermal electrodes (12/18 mm, depending on the muscle, SGM, Ljubiceva, Croatia) inserted into a combination (according to the site of the tumor harbor) of the following muscles on the contralateral side of the body: orbicularis oris, deltoid, biceps brachialis, triceps, extensor digitorum (ED), flexor carpialis (FC), muscles from the tenar eminence, abductor digiti minimi (ADM), tibialis anterior, and abductor hallucis (AH). Filter bandwidth was 50–3,000 Hz, notch off, with a time base of 5 ms/division for upper member and 10 ms/division for the lower, and amplitudes specifically adjusted for every muscle.
Somatosensory-evoked potentials (SSEP) were elicited by electrical stimulation (constant-current) of contralateral median nerve at wrist (upper limb) or posterior tibialis at ankle (lower limb) by 200–300 pulses per train at 7.1 Hz. Pulse duration was 200 μs. Recording through subdermal electrodes was performed at Erb’s point (upper limb) or fossa popliteal (lower limb) and C3’/C4’-Fpz in scalp, bandwidth 10–1,500 and notch off (notch on for recordings at Erb’s point or fossa popliteal).
Cortical somatosensory-evoked potentials (cSSEP) were directly recorded from the grid, with reference electrode placed at contralateral ear lobe, and filters as stated above for SSEP, using the same parameters for stimulation as previously described. For monitoring, we selected the electrode showing a higher amplitude response for N1/P1/N2 potentials.
Transcranial electrical stimulation (TES [17, 27]) was elicited through subdermal electrodes placed 6 cm laterally to midline (C3/C4), used as anode, and cathode placed onto the vertex (Cz). Stimulation by a voltage-constant device was performed by trains of 5–6 pulses at 500 Hz, 50 μs width. Amplitudes were adjusted as low as possible to have a stable response with minimum movement in order to not disturb the surgical dissection. MEPs were recorded through a pair of subdermal electrodes (12/18 mm, depending on the muscle, SGM, Ljubiceva, Croatia) inserted into the following muscles on the contralateral side of the body: orbicularis oris, ED, ADM, tibialis anterior, and AH. Filter bandwidth was 50– 3,000 Hz, notch off, with a time base of 5 ms/division for upper member and 10 ms/division for the lower, and amplitudes specifically adjusted for every muscle. We define the motor threshold as the minimum current required (precision 1 V) to elicit a clear and constant muscle response during TES.
A variant of TES was used in a patient who had a tumor in the left mesial frontal lobe (Fig. 3a). In this case, TES was performed with scalp electrodes placed at both sides of the incision. To preferentially stimulate the frontal medial cortex, the anode was placed 1 cm lateral to the vertex in the direction of the right ear, and a cathode was placed 6 cm laterally to the ipsilateral ear. The rest of stimulation parameters were similar that stated above.
Visual-evoked potentials (VEPs) were obtained by means of light stimulation through goggles at 2.18 Hz, 100 pulses, pulse width 10 ms, bandwidth 10–1,000 Hz, and notch off. Recording using subdermal electrodes placed at O1/O2-Cz (10–20 international system) was performed. Because of the potential phototoxicity induced by 5-ALA, visual stimulation was performed at a basal recording and only when the visual system was potentially at risk.
A combination of these techniques was individually chosen for each patient, considering the tumor location and surgical boarding way. So, for cortical tumors, we used: ECoG (n =14), Cortical SEP mapping (n =14), DCS MEP mapping (n =14), ScS MEP mapping (n =8), DCS MEP and cSSEP monitoring (n =4), or TES MEP and SSEP monitoring (n =4). Meanwhile, for centrum semiovale tumors we used: SSEP and TES MEP monitoring (n =22) and VEPs (n =8). The fibers from the visual system were in danger only when tumors harbored at the centrum semiovale and not when tumors harbored near or in the cortex involving peri-rolandic areas. Therefore, only when tumors harboured in the centrum semiovale were ThCF directed to peri-rolandic and visual areas in danger and, consequently, we monitored both structures so spaced apart.
Surgery
All of the patients orally received freshly prepared solutions of 5-ALA at 20 mg/kg (Medac; Hamburg, Germany) 2–4h prior to the induction of anesthesia. The patients were operated on under general anesthesia, which was induced with a bolus of propofol and remifentanil. The patients were maintained with propofol (5.52 ± 0.30 mg/kg/h; range, 2.5–9.0) and
remifentanil (0.28 ± 0.03 g/kg/min; range, 0.10–1.00). A short-acting muscle relaxant was administered for intubation (succinylcholine, 20–30 mg bolus). Importantly, during the rest of the surgery, no muscle relaxant was administered. Invasive pressure monitoring via an artery was performed, with mean systolic and diastolic pressures of 111.3±4.3 and
56.3±2.7 mmHg, respectively.
The craniotomy and surgery were guided by a neuronavigational system (Brainlab, Feldkirchen, Germany). The tumor was removed using microsurgical techniques, bipolar coagulation, and ultrasonic aspiration. The boundaries of the resection were delimited by the presence of fluorescence, the neuronavigational system and IONM, following the standard warning criteria of amplitude (reduction >50 % for SSEPs or VEPs and >75 % for MEPs) and latencies (retardation >10 %) in the MEPs, SSEPs, or VEPs.
The basal recordings for the MEPs and SSEPs were performed after the dura opening. The basal recording for the VEP was performed several minutes after dura opening but more than 30 min prior to the surgery which may potentially affect the visual system.
When any of the warning criteria appeared, the surgeon always responded by changing the resection area until a complete recovery was observed. If this maneuver did not work, then the surgery was temporally stopped, and the area was irrigated with warm saline. If significant changes in the amplitude and/or latency were consistent and had repeatedly appeared in the same region, irrespective of the presence of fluorescence, then the surgery was terminated.
All of the surgeries were performed by the same neurosurgeon (RGS), and the IONM was performed by the same neurophysiologist (JP) to ensure similar conditions throughout the prospective study.

Statistical analysis
Statistical comparisons between groups were performed using Student’s t test or the Mann–Whitney rank sum test if normality failed. Normality was assessed according to the Kolmogorov-Smirnoff test. Groups that were not normally distributed were subjected to the Kruskal-Wallis one-way ANOVA on ranks. In cases of more than two records per patient, Dunn’s multiple pair-wise comparison method was used.
Pearson’s correlation coefficient was used to study the dependence between variables. A linear regression was calculated by the least square sum. For this linear regression, contrast hypothesis against the null hypothesis ρ=0 used the formula:

which describes a Student distribution with N – 2 degrees of freedom [21].
The statistical significance level was set at p<=0.05. The
results are shown as the means ± SEM, unless otherwise indicated.
Results
IONM in cortical tumors
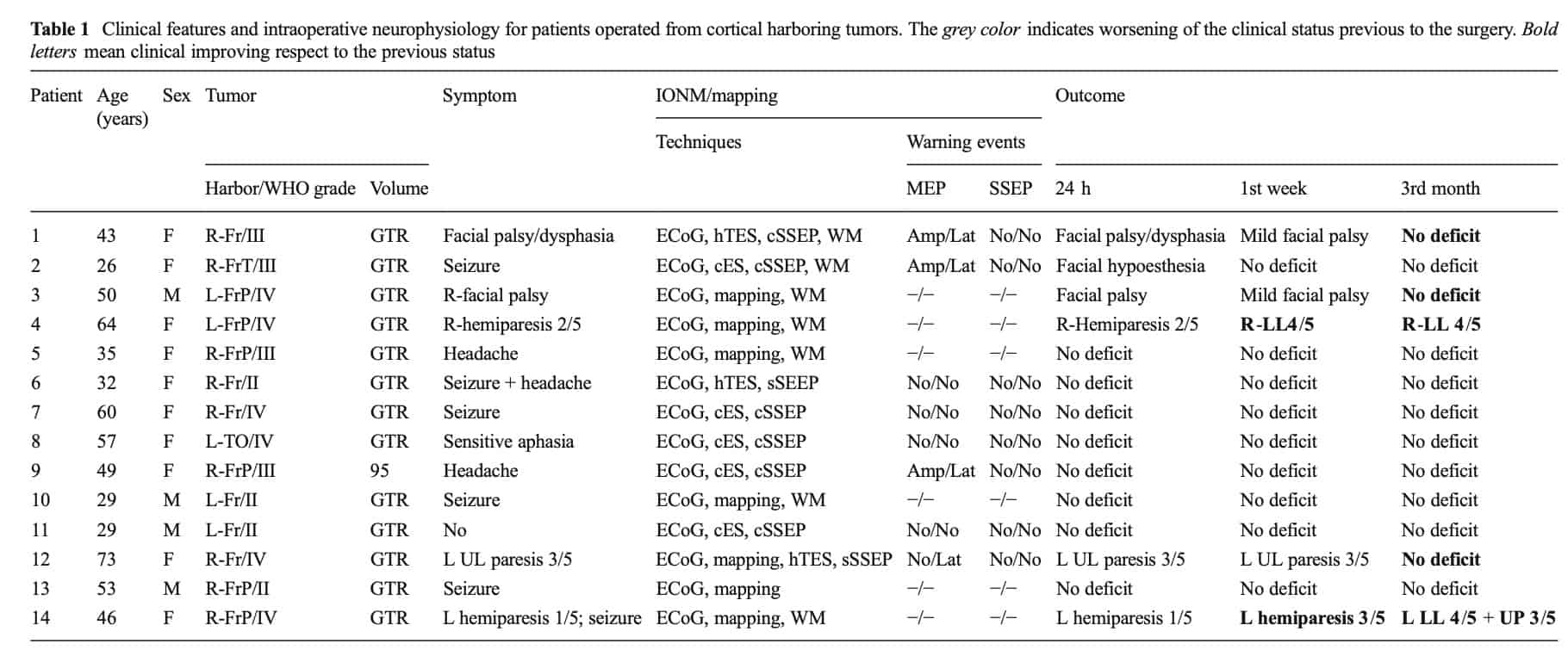
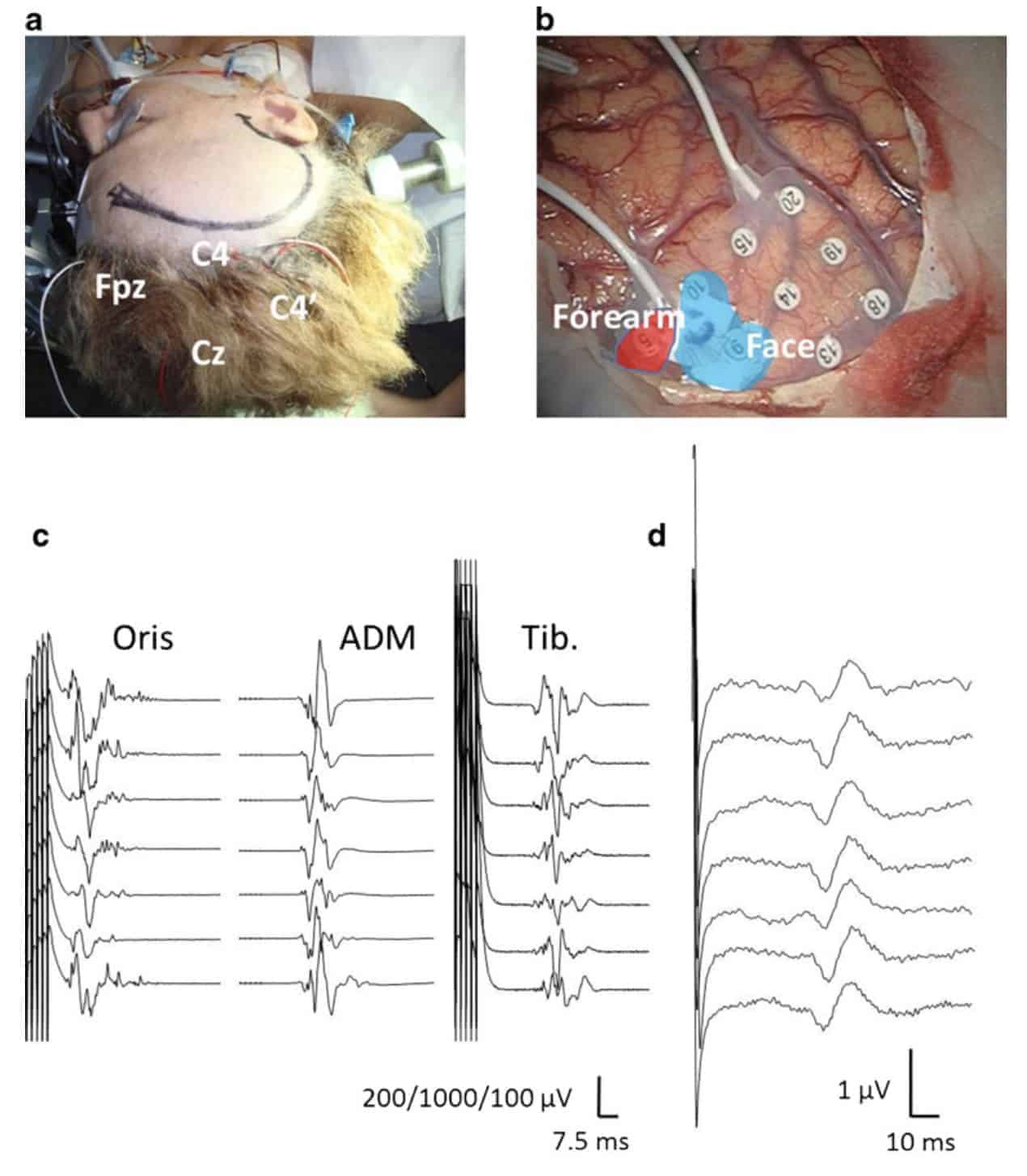
We operated on 13 patients who harbored tumors in or near eloquent cortical areas. As previously stated, all of the patients were operated under complete anesthesia (please refer to Table 1 for further details regarding the clinical features). One of these patients was re-operated on within 9 months, resulting in a total of 14 surgeries. In all of the patients, we performed an ECoG to define the irritative and lesional areas and to monitor the presence of post-discharge during the DCS.
We performed only cortical mapping using cortical electrical stimulation and SSEP (phase-reversal) via a grid in 6/14 cases. In another group of four patients, we continuously monitored the patients by MEP and SSEP, using a grid to stimulate and record after mapping. In the other four patients, after the initial mapping, we monitored the IC by MEPs elicited by TES and the ThCF by SSEPs that were recorded from the scalp.
During the mapping, stimulation through the grid induced a response in the adjacent muscles at the following rates: orbicularis oris 9/12 (in one patient, we also recorded and obtained a response from the intrinsic muscles of the tongue because the tumor was located in the left frontal lobe); biceps brachialis 5/11; triceps 0/7; ED 8/12; FC 10/13; tenar muscles 9/11; ADM 10/13; vasto medialis 1/3; tibialis 2/8 and AH 1/8. The mean motor threshold was 13±2 mA (range, 5–26 mA). No post-discharge or electrical or clinical seizures were observed. At times, we also stimulated via a monopolar probe onto the cortex after removal of the grid. No topographical differences were observed between the two types of stimulation. However, differences in the electrical parameters were not addressed. Surgical incision through the cortex was always selected according to the topography shown for ECoG and cortical mapping.
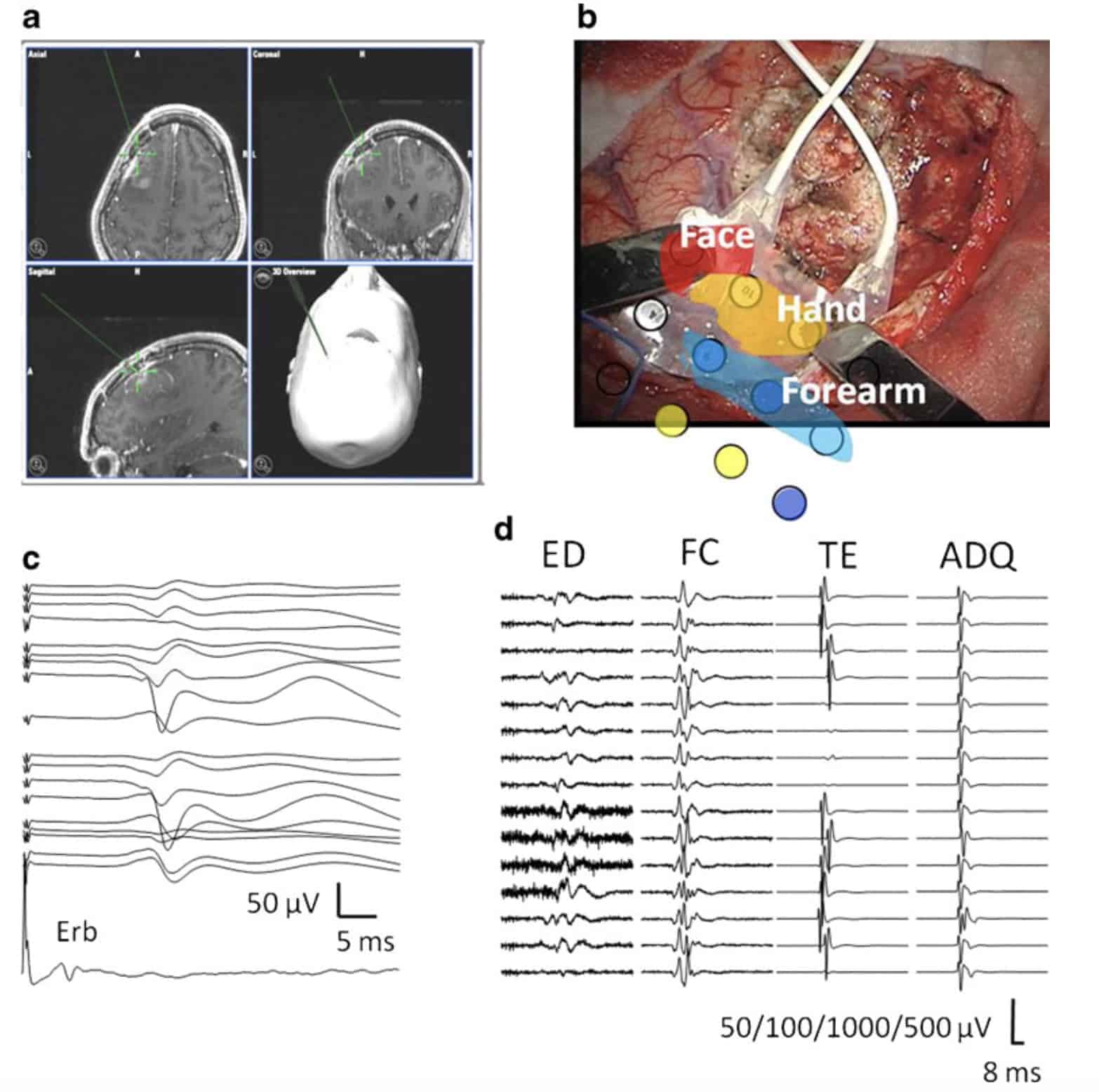
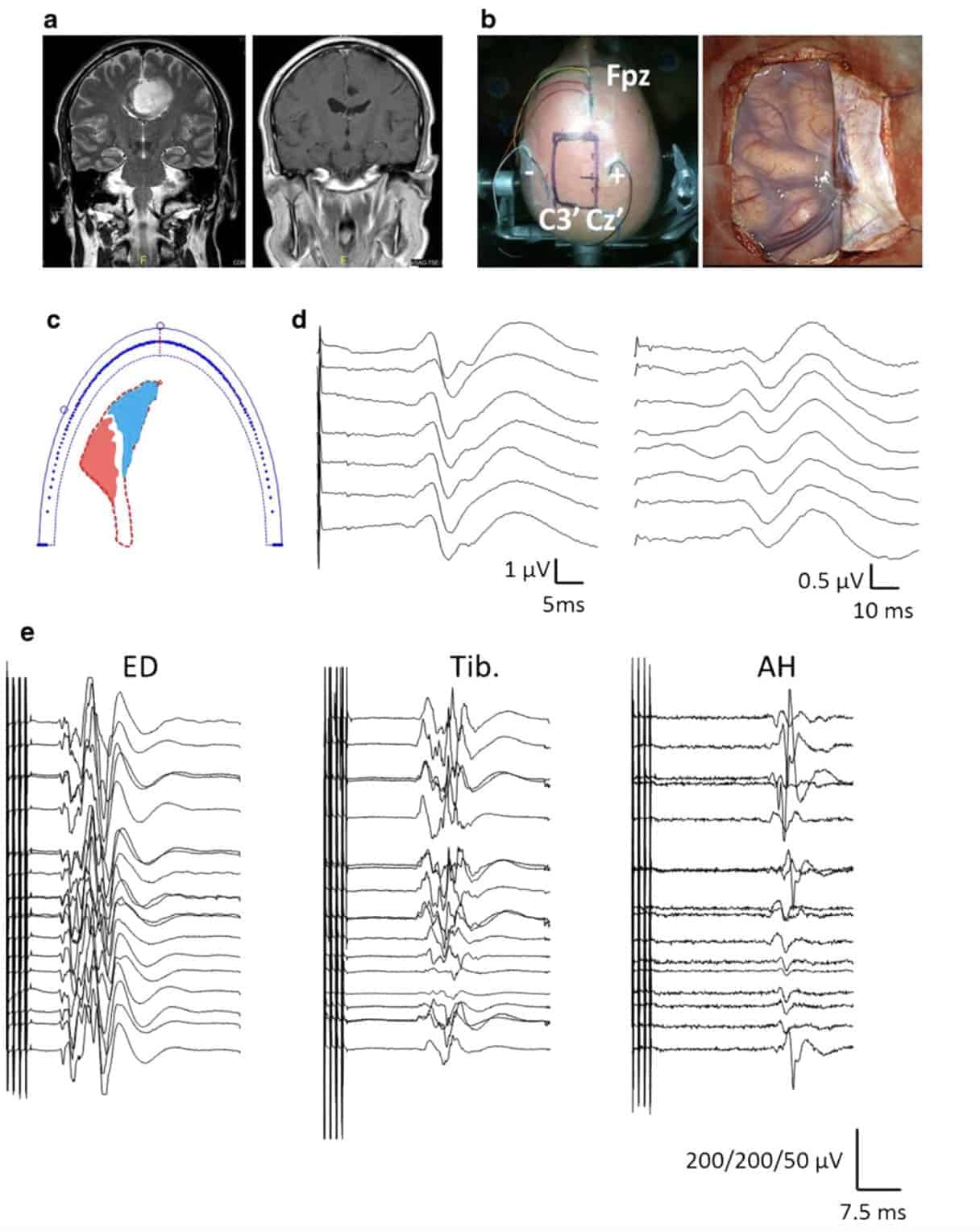
In four patients, we monitored the motor response of the upper limbs and face during the resection by continuous electrical stimulation through the grid (Fig. 1). In four patients, we used hTES to stimulate the IC (see Fig. 2). In these patients, tumor location or the way to access it prevented the placement of a grid for direct cortical stimulation. Therefore, we monitored the motor system via trans-cranial electrical stimulation, taking care to use a configuration of the electric field that induced a response above the level of the resection (see Fig. 2a). In both groups, 3/8 patients exhibited a reduction >50 % and latency >10 % in one or more of the muscles recorded, and in one patient, only an increase in the latency was observed. However, all of these changes were reversible, and no motor neurological deficits appeared after the surgery.
We also performed SSEPs that were recorded using a grid in eight patients. We employed this technique to identify the central sulcus using phase-reversal [2] prior to the motor stimulation. In four patients, we continuously monitored the ThCF function during the resection using this type of recording. In one patient (#2, Table 1), transient facial hypoesthesia was observed in the absence of modifications in the SSEP. However, no new neurological deficits were observed after the surgery in the ThCF system. In four patients, we monitored the ThCF through scalp-recorded SSEPs (Fig. 2).
We stimulated the white matter in eight cases using a monopolar probe. In four patients, we did not obtain any muscular response at 20 mA, which was the maximum intensity examined. However, in the remaining four patients, we obtained a response between 14 and 18 mA.
Amp amplitude <50 % of basal, cES cortical electrical stimulation, cSSEP cortical SSEP, F female, Fr frontal, FrT fronto-temporal, FrP fronto-parietal, hTES hemispheric transcranial electrical stimulation, Lat latency >10 % of basal, LL lower limb, M male, mapping motor cortical stimulation and SSEP to identify phase reversal, No no modification, sSSEP scalp recorded SSEP, TO temporooccipital, UL upper limb, WM white matter stimulation.
Only in one patient (Table 1, #9, 95 % volume resected) we had to stop resection although there was still fluorescence, due to the existence of alarm criteria in motor function. The extension of the resection resulted in a gross total resection in 13/14 patients (92.8 %), and the average resection rate was 97.8 %.
The outcome 24 h after the surgery showed that only one patient demonstrated deterioration compared with their presurgical clinical status. At the end of the first week, two patients showed improvement, and 12 patients exhibited a state similar to their preoperative status. At the end of the third month, five patients showed a clear improvement, and nine patients exhibited a state similar to their preoperative status. None of the patients showed a neurological deficit induced by the surgery.
IONM in tumors located at the semioval center
We operated on 21 patients harboring tumors in the semioval center. One of these patients was re-operated within 7 months, resulting in a total number of 22 surgeries (Table 2). In all of these patients, surgical removal of the tumor was performed far away from the motor cortex, but near to the IC. Thus, direct cortical stimulation was precluded, and trans-cranial electrical stimulation was performed. As previously stated, in all of the patients, monitoring of the motor system was performed using hTES.
We recorded the next muscles, and obtained a response at the following rates: orbicularis oris 19/21; biceps brachialis 4/ 7; ED 21/22; FC 1/2; tenar muscles 3/3; ADM 21/22; tibialis 12/20 and AH 15/22. The mean motor threshold was 214± 13 V (range, 100–320 V). This low voltage level enabled an adequate motor stimulation during microdissection, resulting in no disturbances to the surgeon.
In one patient who had a tumor in the left mesial frontal lobe (Fig. 3a), TES was performed with scalp electrodes placed at both sides of the incision. This patient deserves further attention. To preferentially stimulate the frontal medial cortex, an anode was placed 1 cm lateral to the vertex in the direction of the right ear, and a cathode was placed 6 cm laterally to the ipsilateral ear. Theoretical consideration regarding the different excitation areas in the IC with the anode position is shown in Fig. 3c. The motor stimulation obtained showed a reliable and reproducible pattern response in the upper and lower contralateral limbs during most of surgery. This pattern continued until a sudden decrease affected only the lower limb, whereas a normal response was elicited from the muscles of the face and upper limb (Fig. 3e). This selective change was reversed when the surgeon moved to a different area of the resection. Thus, the TES stimulated directly in or near the cortex because changes in the motor function of the lower limb correlated well with the surgical action on the medial frontal cortex.
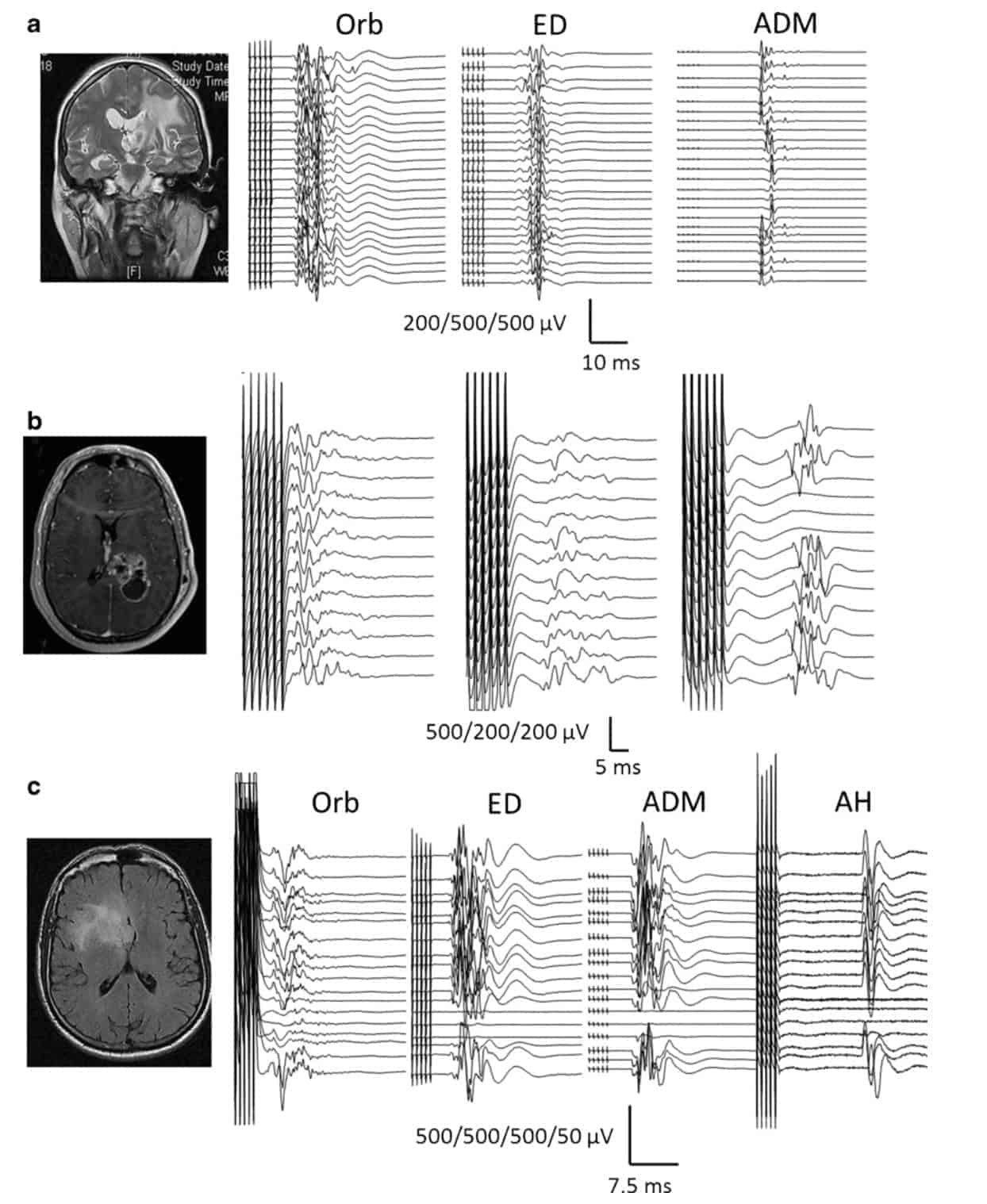
We observed a reduction in the amplitude of >50 % and an increase in latency of >10 % in one or more muscles in 14/22 patients, and in three patients, we observed an increase in the latency alone. Interestingly, warning criteria occurred in isolated muscles (segmental modifications) (Fig. 4). These segmented changes were the most commonly observed, appearing in 13 cases. Changes in all of the recorded muscles were observed in only one patient (see Fig. 4c). The appearance of segmental modifications in the motor response was considered as a sign of danger, which required safety measures. In 11/14 patients, these changes were reversible, and no new motor neurological deficits appeared after the surgery. However, in three patients (#3, 8, and 11, Table 2), a severe alteration in the motor response was observed.
In the SSEP recordings, we observed significant changes in the amplitude and latency in 1/22 surgeries. This patient also showed a global affectation in motor response. The modification of the motor conduction was reversible; however, this was not the case in the ThCF, where the modifications persisted at the end of the surgery. A transient change in the SSEP latency was observed in one patient, and a decrease in the amplitude was observed in four patients.
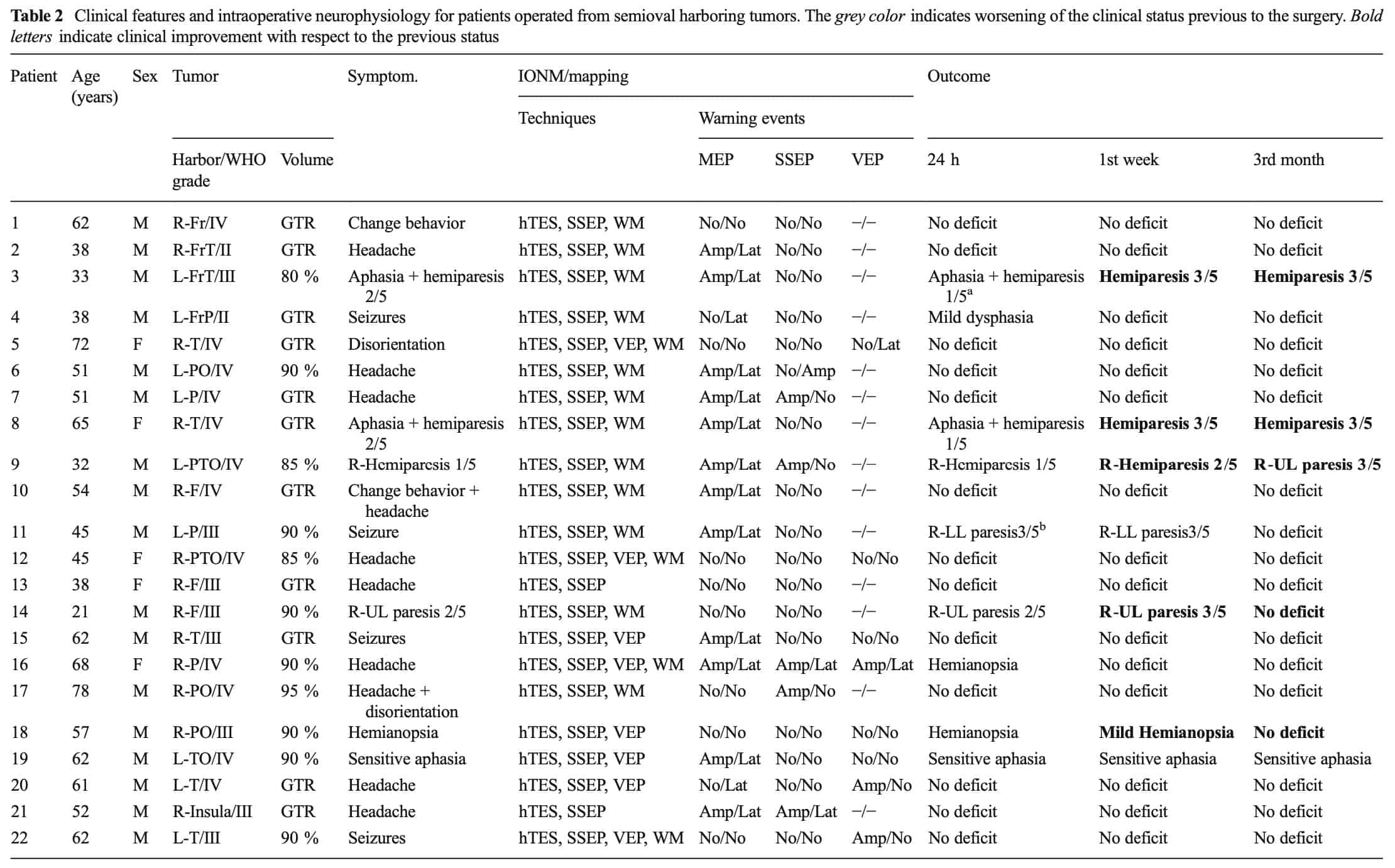
Amp amplitude <50 % of basal, cES cortical electrical stimulation, F female, Fr frontal, FrP fronto-parietal, FrT fronto-temporal, hTES hemispheric transcranial electrical stimulation, Lat latency >10 % of basal, LL lower limb, M male, No no modification, P parietal, PO parieto-occipital, PTO parieto-temporo-occipital, SSEP scalp recorded SSEP, T temporal, TO temporo-occipital, UL upper limb, WM white matter stimulation a Intraventricular bleeding after the surgery b Venous infarction after the surgery.
In eight patients, we monitored the visual system using VEP. In 4/8 patients, we observed significant changes in either the amplitude or latency, and in another patient, a combined change in the latency and amplitude was observed. In the last patient (#15, Table 2), a transient visual deficit was observed after the surgery. Although 5-ALA exhibits significant photo-toxicity, it is important to note that no visual alterations were reported due to phototoxicity. Nevertheless, the number of trains of the VEP was limited.
In this group of patients, surgery was stopped despite the presence of fluorescence in three cases (Table 2, #6, 11, and 16, 90% volumes resected). In two of these cases, a transient neurological deficit was observed.
The extension of the resection resulted in a gross total resection of 11/22 patients (50.0 %), and the average resection rate was 93.3 %.
When we examined the outcome 24 h after surgery, five patients showed a clinical deterioration. However, at the end of the first week, only one patient maintained a poor clinical score, and five patients showed improvement. Furthermore, at the end of the third month, five patients showed a clear improvement. The rest of the 17 patients exhibited a similar pre-surgery state. Similar to the cortical surgery group, at this time, no patients showed any neurological deficit after the surgery.
Discussion
In this study, we have shown that it is possible to obtain a significant percentage of GTR (66.7 %), with a mean tumor resection of 90.4±3.7 % in patients harboring tumors in or near eloquent areas during FGR surgery with absence of neurological deficits. In addition, a significant percentage of patients exhibited clinical improvement after the surgery (27.8 %). This is an important result in patients with a deceptively short life expectancy because there is promise of an adequate quality of life.
During resection, we have observed significant changes in IONM repeatedly. Considering these modifications as warning signals, we have used them to modify the surgery and this enable us termination prior to the induction of permanent neurological deficits.
FGR enables the performance of a complete resection in 65 % of patients compared to only 36 % in non-FGR surgeries [23]. However, an elevated degree of neurological alterations after the surgery [3] was observed due to the difficulty in the identification of functional areas and tracts during operation. Furthermore, the risk of neurological deterioration was higher in patients who did not respond to steroids, most likely because the tumor was intermingled with the functional tissue and was not derived from edema [26]. Thus, it is extremely important to identify the actual boundaries of the functional tissue, particularly when fluorescence infiltration is observed. Other various approaches have been used to avoid neurological deficits, which combine intraoperative MRI with FGR [28] or MRI with IONM [20]. However, in the latter case, it is difficult to understand how morphological studies can identify functionally significant structures such as eloquent cortical areas or tracts.
In patients who harbor tumors in the cortex, we used general anesthesia. Within recent years, there has been a renewal in the use of awake craniotomies [4, 13, 14, 19]. No differences in the immediate postoperative motor status, extent of resection, or threshold intensity were found when both methods were compared [13]. In our study, no neurological deficits were observed in the anesthetized patients, and thus, we proposed that surgery near cortical eloquent areas can be performed safely when intensive neurophysiological mapping and monitoring are also employed [18]. Moreover, this combined approach will be much more comfortable for both the patient and surgical team.
5-ALA exhibits phototoxicity [8], for which reason the patients must wear a facial mask and stay in the darkness for 24 h. Thus, the use of VEPs, which can be elicited by flashes, may be potentially dangerous. With this idea in mind, we restricted the number of light stimulations to be as low as possible. Fortunately, none of the eight patients that required a VEP for the IONM indicated new visual alterations after the surgery due to phototoxicity. Additional data are required before a safety level of VEP and FGR surgery may be established; however, a margin may be determined to monitor the visual system without iatrogenic deterioration.
Hemispheric TES has been used to stimulate the motor system in surgeries near the cortex. We did not find any falsenegative cases, and the observed changes in motor function were reversible most of the time when the surgeon moved to a different place or stopped the manipulation. In cases where the motor function did not completely recover, a transient motor deficit was observed. Previous studies have shown that the sensitivity and specificity for this type of stimulation were similar to thTES [17], and although this study did not address this aspect, our results confirm its utility. The voltage used was sufficiently low to enable stimulation during the microdissection because there were no significant movements. This was a very important feature because provided practical knowledge of motor function in real time. In addition, the pattern of activated muscles was broader compared to the cortical stimulation on the motor strip. In the latter case, the area just beneath the grid electrodes could be stimulated, and usually it is very difficult to place a grid/strip that would cover the patient from the face to the shoulder. However, hTES consistently elicited a response in the upper limb and to a higher degree compared to cortical stimulation of the face and lower limb. Nevertheless, there was a real potential risk of error when the voltage was too high or when the surgery was performed above the area of stimulation. In these cases, the hTES was replaced by cortical stimulation, if possible, which reinforced the awareness of the limitations.
Our main clinical goal was to resect as much as possible without neurological deficit. Consequently, we did not address the specificity and sensitivity of the IONM. In contrast, we used classical warning thresholds, assuming that sustained modifications indicated a greater probability of neurological deficit [26]. However, it has been shown that changes in the latency and amplitude of cortical MEP recordings serve as warning criteria in addition to providing prognostic values in IONM during surgery in the vicinity of the IC [7]. It is very important to take into account that in four patients surgery was stopped after severe warning criteria, despite the presence of remaining fluorescence. In all of these cases, no permanent neurological injury was observed, although transitory alterations were seen in two of them. The decision to stop the surgery was adopted following the criterion indicated above to preserve neurological function over the presence of fluorescence. We did not find any false-negatives in the motor or sensory functions in patients with neurological deficits at 24 h. However, patient #2 (Table 1) demonstrated facial hypoesthesia. Nevertheless, the SSEPs monitored the function of the upper limb and did not show any alterations, particularly in the face. Most likely, monitoring of trigeminal SSEPs is required in such cases.
In patients with tumors located in the semioval center, no false-negative responses were observed. In three patients, transient motor deterioration changes in the IONM were observed. In patient #4 (Table 2) a mild deterioration of language was observed. This deterioration was recovered within a few days and was most likely induced by an alteration in the arcuate fasciculus and not in the cortical eloquent areas. The only patient with a greater discrepancy between the results of the IONM and motor function was patient #11 (Table 2). In this patient, the motor function had immediately returned after the patient recovered from the anesthesia; however the patient suffered from a venous infarction within the first 12 h, and his motor function had deteriorated. Nevertheless, the patient had completely recovered at delivery.
In both groups of patients, those who were operated on at the semioval center and at the cortex, a greater number of transient neurological alterations (18.2 and 7.1 %), lower percentage of GTR (59.1 and 92.8 %) and resected volume (93.3 and 97.8 %) were observed in semioval surgery compared to cortical surgery. In addition, the percentage of warnings in either the motor or somatosensory recordings was higher in the semioval surgery (68.2 and 50.0 %, respectively). It has been shown that vascular dynamics such as vasospasm or congestive edema can cause changes in the MEP response [12, 26]. In our study, transient changes in motor function were observed with relative frequency. Most likely, this vascular effect is involved in a larger number of warning events and, consequently, carries a praecox stop in surgery with a lower percentage of resection.
By conclusion, FGR is a powerful technique developed to help the neurosurgeon improve the degree of tumor resection. However, is it extremely important to identify the functional limits of the resection to ensure an adequate quality of life. We have shown in this study that IONM can be helpful during surgery to avoid neurological deficits and to improve the quality of life in these patients.
Acknowledgment
This work was supported by a grant from the Plan Nacional de Investigación Científica, Desarrollo e Innovación Tecnológica (I + D + I), Instituto de Salud Carlos III, Subdirección General de Evaluación y Fomento de la Investigación PI12/02839.
Conflicts of interest
None.
References
1. Bello L, Gambini A, Castellano A, Carrabba G, Acerbi F, Fava E, Giussani C, Cadioli M, Blasi V, Casarotti A, Papagno C, Gupta AK, Gaini S, Scotti G, Falini A (2008) Motor and language DTI fiber tracking combined with intraoperative subcortical mapping for surgical removal of gliomas. Neuroimage 39:369–382
2. Cedzich C, Taniguchi M, Schäfer S, Schramm J (1996) Somatosensory-evoked potential phase reversal and direct motor cortex stimulation during surgery in and around the central region. Neurosurgery 38:962–970
3. Díez R, Tejada S, Idoate MA, García de Eulate R, Domínguez P, Aristu J (2011) Surgery guided by 5-aminolevulinic fluorescence in glioblastoma. Volumetric analysis of extent of resection in single center experience. J Neurooncol 102:105–113
4. Duffau H, Capelle L, Sichez J, Faillot T, Abdennour L, Law Koune JD, Dadoun S, Bitar A, Arthuis F, Van Effenterre R, Fohanno D (1999) Intra-operative direct electrical stimulations of the central nervous system: the Salpetrier experience with 60 patients. Acta Neurochir (Wien) 141:1157–1167
5. Feigl G, Ritz R, Moraes M, Klein J, Ramina K, Gharabaghi A, Krischek B, Danz S, Bornemann A, Liebsch M, Tatagiba MS (2010) Resection of malignant brain tumors in or near eloquent cortical areas: a new multimodal approach combining 5-aminolevulinic acid and intraoperative monitoring. J Neurosurg 113:352–357
6. Kamada K, Todo T, Ota T, Ino K, Masutani Y, Aoki S, Takeuchi F, Kawai K, Saito N (2009) The motor-evoked potential threshold evaluated by tractography and electrical stimulation. J Neurosurg 111:785–795
7. Kombos T, Suess O, Funk T, Kern BC, Brock M (2001) Monitoring of intraoperative motor-evoked potentials to increase the safety of surgery in and around the motor cortex. J Neurosurg 95:608–614
8. Krammer B, Plaetzer K (2008) ALA and its clinical impact, from bench to bedside. Photochem
Photobiol Sci 7(3):283–289
9. Krieg SM, Shiban E, Droese D, Gempt J, Buchmann N, Pape H, Ryang YM, Meyer B, Ringel F (2012) Predictive value and safety of intraoperative neurophysiological monitoring with motor-evoked potentials in glioma surgery. Neurosurgery 70(5):1060–1071
10. Morofuji Y, Matsuo T, Hayashi Y, Suyama K, Nagata I (2008) Usefulness of intraoperative photodynamic diagnosis using 5-aminolevulinic acid for meningiomas with cranial invasion: technical case report. Neurosurgery 62(3 Suppl 1):102–104
11. Pastor J, Pulido P, López A, Sola RG (2010) Monitoring of motor and somatosensory systems in a 26-weeks pregnant woman. Acta Neurochir (Wien) 152:1231–1234
12. Neuloh G, Pechstein U, Scharmm J (2007) Motor tract monitoring during insular glioma surgery. J Neurosurg 106(4):582–592
13. Nguyen HS, Sundaram SV, Mosier KM, Cohen-Gadol AA (2011) A method to map the visual cortex during an awake craniotomy. J Neurosurg 114(4):922–926
14. Nossek E, Korn A, Shahar T, Kanner AA, Yaffe H, Marcovici D, Ben-Harosh C, Ben Ami H, Weinstein M, Shapira-Lichter I, Constantini S, Hendler T, Ram Z (2011) Intraoperative mapping and monitoring of the corticospinal tracts with neurophysiological assessment and 3-dimensional ultrasonography-based navigation. J Neurosurg 114:738–746
15. Ozawa N, Muragaki Y, Nakamura R, Hori T, Iseki H (2009) Shift of the piramidal tract during resection of the intraaxial brain tumors estimated by intraoperative diffusion-weighted imaging. Neurol Med Chir 49:51–56
16. Pastor J (2011) Neurofisiología Intraoperatoria. In: Navarrete EG, y Sola RG (eds) Neurocirugía Funcional y Estereotáxica. Viguera Editores, Barcelona, pp 589–604
17. Pastor J, Perla y Perla P, Pulido P, Sola RG (2010) Hemispheric transcranial electrical stimulation: clinical results. Rev Neurol 51(2):65–71
18. Pastor J, Pulido P, Sola RG (2013) Neurophysiological assisted transsulcal approach to a high-grade glioma without affect neither motor nor somatosensory function. Rev Neurol 56(7):370–374
19. Peruzzi P, Puente E, Bergese S, Chiocca EA (2011) Intraoperative MRI (ioMRI) in the setting of awake craniotomies for supratentorial glioma resection. Acta Neurochir Suppl 109:43–48
20. Senft C, Forster M-T, Bink A, Mittelbronn M, Franz K, Seifert V, Szelényi A (2012) Optimizing the extent of resection in eloquent located gliomas by combining intraoperative MRI guidance with intraoperative neurophysiological monitoring. J Neurooncol 109:81–90
21. Spiegel MR (1991) Teoría de la correlación. In: Spiegel MR (ed) Estadística. McGraw-Hill Interamericana, Madrid, pp 322–356
22. Stepp H, Beck T, Pongratz T, Meinel T, Kreth FW, Tonn JC (2007) ALA and malignant glioma: fluorescence-guided resection and photodynamic treatment. J Environ Pathol Toxicol Oncol 26:157–164
23. Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ (2006) Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomized controlled multicenter phase III trial. Lancet Oncol 7:392–401
24. Stummer W, Reulen HJ, Novotny A, Stepp H, Tonn JC (2003) Fluorescence-guided resections of malignant gliomas–an overview. Acta Neurochir Suppl 88:9–12
25. Stummer W, Stocker S, Wagner S, Stepp H, Fritsch C, Goetz C, Goetz AE, Kiefmann R, Reulen HJ (1998) Intraoperative detection of malignant gliomas by 5-aminolevulinic acid-induced porphyrin fluorescence. Neurosurgery 42:518–526
26. Stummer W, Tonn J-C, Mehdorn M, Nestler U, Franz K, Goetz C, Pichlmeier U, ALA-Glioma Study Group (2011) Counterbalancing risks and gains from extended resections in malignant glioma surgery: a supplemental analysis from the randomized 5-aminolevulinic acid glioma resection study. J Neurosurg 114:613–623
27. Szelényi A, Kothbauer KF, Deletis V (2007) Transcranial electric stimulation for intraoperative motor-evoked potential monitoring: stimulation parameters and electrode montages. Clin Neurophysiol 118:1586–1595
28. Tsugu A, Ishizaka H, Mizokami Y, Osada T, Baba T, Yoshiyama M (2011) Impact of the combination of 5-Aminolevulenic acid-induced fluorescence with intraoperative magnetic resonance imaging-guided surgery for glioma. World Neurosurg 76(1/2):120–127