FCD- Focal Cortical Dysplasia
Servicio de Neurocirugía
Hospital de la Princesa
Introduction
Focal cortical dysplasia (FCD) is the most commonly encountered developmental malformation causing refractory epilepsy. This is a malformative lesion of the brain due to an alteration of the normal process of cortical development. But before focusing in developmental malformations I think we should talk a little about neocortical malformations in general. In Engel’s book of Epilepsy, he describes these neocortical malformations as a heterogeneous group that can be roughly categorized as:
-
• Cortical dysplasia: these are the majority of malformations associated with pediatric epilepsy and include the full spectrum of neuronal migration disorders.
• Structural lesions associated with tuberous sclerosis complex.
• Sturge Weber syndrome
• Neurofibromatosis type 2 associated with meningo-angiomatosis.
• Vascular malformations.
Developmental malformations of the neocortex can be considered a spectrum of cortical dysplasia resulting from derangement of the normal process of cortical development. As we have said cortical dysplasia is one of the most important causes of developmental malformation of the neocortex that includes a range of morphologic features, from the most subtle (microdysgenesis) to the most severe (hemimegalencephaly) and others like agyria, polimicrogyria or focal cortical dysplasia, and that are associated with multiple etiologic factors.
Malformations of cortical development produce drug-resistant epilepsy in 76% of the cases, and it is the etiology of drug-resistant epilepsy in 15-20% of adult patients and over 50% of pediatric patients. The most common type of these malformations is focal cortical dysplasia.
This term was used for specific lesions with cytomegalic neurons, after Taylor’s description in 1971. However the nomenclature of cortical dysplasia has evolved through several classifications as sometimes it is ambiguous and some investigators prefer the traditional classification of migration disorders divide them in four groups: agyria/pachygiria-lissencephaly, microgyria-polymicrogyria, displasic cortical architecture and heterotipias. Due to its pathophysisology other authors call it neural migration disorders. Finally there have been a recent consensus with a proposal to subclassify cortical dysplasia using a morphologic criteria that it’s known as Palmini classification.
Focal cortical dysplasia appears, as other malformations of cortical development, as a result of an insult in a rapidly developing brain. Neocortical formation starts after the neural tube formation and have different steps that could be briefly summarize as:
-
• cell proliferation in the ventricular zone and subventricular zone (VZ/SVZ)
• early differentiation of neuroblasts and glioblasts
• program cell death of neuronal precursors and neurnons
• migration of neuroblasts to form the cortical plate
• late neuronal migration
• organization and maturation of the cortex
• synaptogenesis
Abnormalities of these processes results in abnormalities of cortical architecture and its electrophysiologic properties. Most developmental disorders of the brain associated with epilepsy are believe to originate from the perturbation of developmental events the embrionyc period (around 6 weeks of gestation) due to multiple causes. In Table 1 we could see that focal cortical dysplasia appears due to alterations in the fetal period as a result of problems in the neuronal and glial proliferation or in the perinatal period because of problems in the organization of the cortex.
ETIOLOGY
Many authors consider this abnormalities that produce FCD can be attributed to a combination of environmental and genetic factors. Some genes named to be implied in FCD are TSC 1 or TSC 2, and actually some authors consider FCD as a form of tuberous sclerosis without extracerebral symptoms. Changes in proteins of Wnt or Notch signaling pathway have been also proposed as them are involved in a proper neuronal migration.
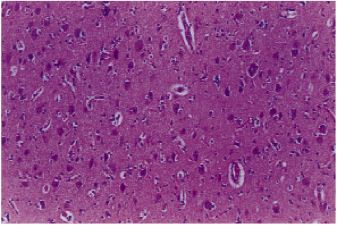
So focal cortical dysplasia is characterized for two types of alterations:
-
• Cortical architecture abnormalities: this could be columnar disorganization (formation of vertically oriented microcolumns consisting of at least 8 neurons) and laminar disruption (alterations in 6-layered composition of the cortex)
• Cytological abnormalities:
- o Hypertrophic neuron cells outside typical location in layer V
Hypertrophic neuron cells
Immature neurons
Dysmorphic neurons
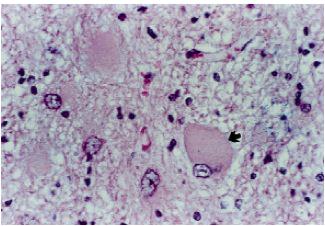
Balloon cells
o Immature neurons round or oval cells with large nucleus and thin rim of cytoplasm, absent in mature cortex.
o Dysmorphic neurons with abnormal size and morphology of axons and dendrites, as well as increased accumulation of neurofilament proteins.
o Balloon cells which are pathognomonic for Taylor dysplasia and consist in large cells with an ill membrane, single or multiple eccentric nuclei and eosinophili cytoplasm, demonstrating immunohistochemical features of neuronal and glial linneage.
According with this type of histological abnormalities, nowadays we can classify focal cortical dysplasia based on Palmini’s classification:
-
• Type I or benign characterized by isolated architecture abnormality, which is divide in two types depending on the presence of abnormal cells (such as hypertrophic on immature neurons, Type Ib) or not (type Ib)
• Type II. This was the first type described by Taylor encompassing larger abnormalities with dislayering and additional presence of dysmorphic neurons (ballon cells) in type IIb.
After the observation that FCD was frequently found in hippocampal atrophy, neoplasic developmental tumors (DNET) or in posttraumatic and postischemic patients, in 2012 appeared a new classification by Blumbcke and other experts that modified the one by Palmini which differentiates between three groups of FCD:
-
• Type I malformations presenting abnormal cortical layering as a result of abnormal radial migration and maturation of neurons (Ia) or disruption of typical 6 layered tangencial composition of the cortex with immature neurons (Ib) or compromising both architectural abnormalities (Ic)
• Type II malformation resulting from disrupted cortical lamination and specific cytological abnormalities. Type IIa with dysmorphic neurons and type IIb with dysmorphic neurons and balloon cells.
• Type III malformations connected with different cortical dislamination and cytological abnormalities with main lesion within the same area or lobe. In type IIIa cortical dyslayering was associated with hippocampal atrophy, IIIb with glial or glioneuronal tumors (DNET, ganglioglioma), IIIc with vascular malformations (AVMs, hemagiomas, telangiectasias), IIId acquired at early age (trauma, ischemia or perinatal hemorrhage, infectious or inflammatory diseases) and other non-classified.
Clinical
Patients with FCD have a heterogeneous clinical picture that can present in almost any type and at any age. Although there are no clinical features that are specific for FCD, there are some factors that create a strong suspicion to think about it. These factors include an association with developmental delay and static focal neurologic deficits, frequent seizures from an early onset or focal status epilepticus.
The severity of seizures also varies enormously. There are some individuals with large FCD who have relatively few seizures and on the other hand there are some individuals with relatively small FCD who have very severe and intractable epilepsy.
Seizures usually star in the first decade after age 2 to 3 years, but there are some patients with seizure onset in the sixth decade. Patients with FCD type II manifest earlier onset comparing to type I. Similarly earlier onset is observed in patients with a larger focus on brain MRI as compared to patients with smaller lesions.
Seizures could be of many different types, simple or pure motor seizures, complex partial seizures, or secondary generalized are common. Usually seizures often occur in clusters.
According to the literature FCD type I is related to temporal lobe seizures. In patients with FCD type II, multilobar lesions are found, involving hemisphere, often with extratemporal location and mainly in the frontal lobe. Therefore seizures with early onset in neonatal period or childhood are more likely FCD type II with multilobar or hemispheric lesion, while FCD type I with a small focus, usually in the temporal lobe, predominates in adults.
EEG Study
The interictal scalp electroencephalogram (EEG) may demonstrate focal-ictal like activity over the dysplasic lesions, underscoring their high epileptogenicity. However there is no clear correlation between the interictal EEG and imaging features in FCD. In patients with FCD EEG studies have reported continuous epileptform discharges which correlates with greater surgical success. The intrinsic hyperexcitability of abnormal cortex in FCD has been confirmed in numerous studies, associated to a fast propagation from neocortex to mesial temporal regions.
Ictal EEG studies have suggested that FCD is a neural network disorder with secondary ictal zones. Intraictal activation is typical of FCD and can be contiguous or at a distance from the primary epileptogenic area.
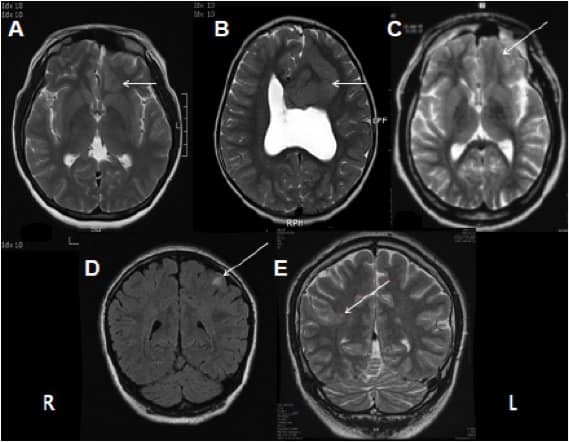
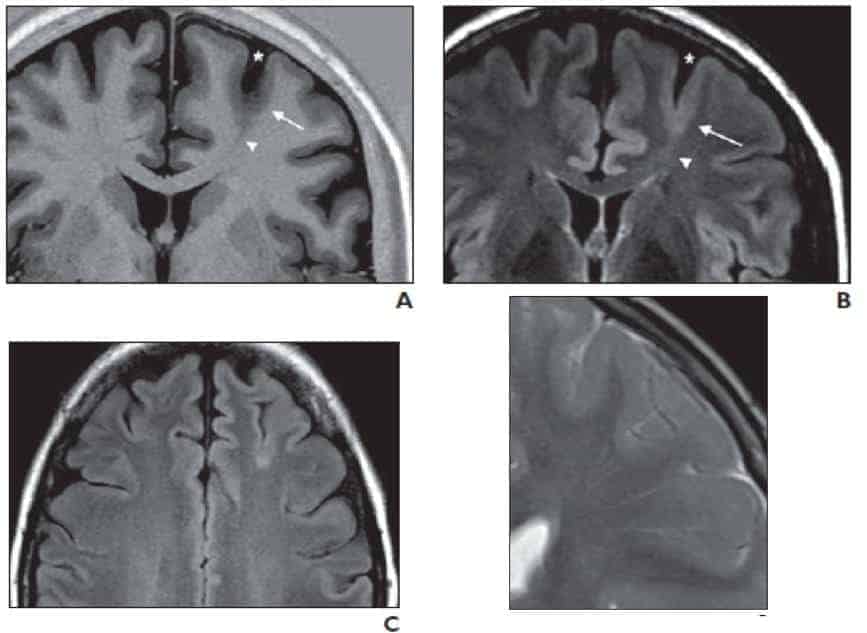
Image Study
To diagnose FCD, we should have a brain MRI with the characteristic features of FCD. The classical MRI findings consist of abnormal gyral thickening and abnormal gyral architecture with or without underlying T2-weighthed gray and white matter changes. Focal increased signal in T2 or FLAIR and blurring gray-white matter can also be observed. The transmantle sign consists in an increased signal from the cortical surface to the ventricle. These changes can be circumscribed in nature but can be extensive, involving more than one gyrus or lobe. High-resolution MRI with thin slides and multiplanar reconstruction are often necessary to make the diagnosis. Also concomitant use of T2 and FLAIR imaging are important in detecting small FCD.. Thirty seven percent of the patients with type I FCD had normal MRI while only 15% with type II FCD had negative MRI. The thick gray matter, blurring gray and white matter junction and increased T2 and FLAIR signal are more frequently associated with type II FCD. However, most MRI findings could not differentiate type I and type II pathology because of significant overlapping of imaging findings between both of them.
Cortical thickness and blurring o gray-white junction were more common in isolated FCD than in FCD type III. And transmantle sign on MRI was more specific to type II.
Abnormal gyral architecture
Focal increased signal in T2 or FLAIR
Blurring in T2 or FLAIR
Transmantle sign
There are two subtypes of FCD which could be differentiate by MRI. Transmantle cortical dysplasia appears in patients with epilepsy onset from infancy to early adulthood. On MRI the imaging abnormality extends radially from the cortical surface to the lateral ventricule. The lesions are most often small, but a few patients have large abnormalities with abnormal cortical gyration. It is thought that this particular malformation stems from a disorder affecting the radial-glial neuronal unit.
On the other hand bottom of the sulcus appears as a highly epileptogenic lesion with an excellent prognosis for seizure control following focal resection. The most common imaging findings are typical of FCD with a very small lesion that can be restricted to the bottom of the sulcus. A characteristic feature of bottom of the sulcus dysplasia is the funnel-shaped structure directed towards the ependymal surface, presented in most cases. Histological features are identical to those of typical FCD. The absence of gross gyration abnormalities is also tyical of bottom of sulcus dysplasia. Furthermore, the postsurgical outcome is excellent sine the lesions are often very small and surgically accessible.
The severer pathology might mean the higher epileptogenicity in FCD. However, the most severe pathological presentation can be found in patients with negative MRI. But the diagnostic sensitivity is increased along with the severity of pathology of FCD. The proportion of negative MRI in the patients with pathologically proven FCD ranges from 23-73% in different series.
Ictal SPECT and FDG-PET can be critical for localizing the seizure focus, especially in MR negative patients. A study by Schawrt et al involving 462 cases showed that 32% of normal MRI were associated with abnormal PET imagings. For cortical dysplasia, the diagnostic sensitivity of FDG-PTE and ictal SPECT ranges from 69% to 98% and 48% to 64% respectively.
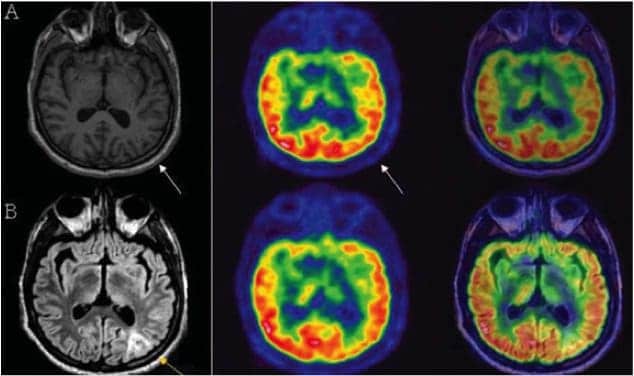
In these images we can see a local or regional zone of hypometabolism corresponding to a single gyrus or a cortical region depending on the lesion.
There are some new techniques for imaging diagnose of FCD. A new type of sequence called NODDY (neurite orientation dispersion and density imaging) is an advanced diffusion imaging sequence that provides additional information on tissue microestructure, including intracellular volume fraction, a marker of neurite density. In a study made by Winston et al they applied this sequence on 5 patients, and conclude that NODDY may assists the clinical identification of FCD in patients with epilepsy that is not easily seen on other imaging sequences and requires further study. In this images we could see a hypointense zone that correspond to the FCD.
ICVF a marker of neurite density.
NODDY may assists the clinical identification.
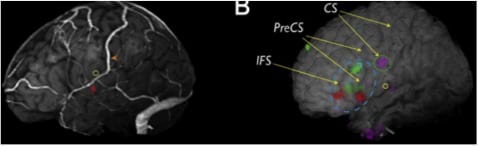
Yang et al have also published 6 cases in which they have used three-dimensional brain surface visualization for FCD surgery. These images allowed the surgeon for topographic understanding of the lesion in relationship to eloquent tissue, anatomic landmarks and surface veins.
Stereo-EEG
Also to complete the study intracranial EEG can be performed if methods described before are insufficient to determine the epileptogenic focus. This is often required especially in cases of negative MRI or discordant MRI and video EEG. Enatsu et al have also proponed a combination between SEEG and subdural electrodes as SEEG can only sample isolated cortical areas with the inability to record contiguous cortical regions that may cause difficulties in interpretation. According to the authors this hybrid technique subdural strip provided information regarding the precise description of seizure spread in the cortical surface, more preface definition of functional cortex and a better delineation of the interface between epileptogenic zones and functional cortex.
Treatment
As we have talked before, epileptic seizures due to FCD are difficult to control with pharmacological treatment and often intractable. According to this, surgical treatment appears to be the next therapeutic procedure, which could be made by resection of the lesion, lobectomies or even hemispherectomies in some cases. More limited surgeries are performed in elderly patients, usually due to FCD type I, usually located within the temporal lobe. Younger patients usually have FCD type II, with more extensive lesions and extratemporal location, predominantly in the focal areas. In these cases operation includes lobectomy or even hemispherectomy.
The proportion of FCD in surgical series ranges from 9% to 71% depending on the selection criteria. Yun et al published in 2006 a study with one hundred ninety-three patients with neocortical epilepsy in which 71% of the presented FCD.
It exist a poorer outcome of FCD surgery compared with other pathologies such as benign brain tumors or temporal lobe epilepsy with hippocampal sclerosis. Whereas approximately 80% of patients became seizure free after surgical treatment for mesial temporal lobe epilepsy related to hippocampal sclerosis or lesional epilepsy, the efficacy of surgical treatment for FCD was consistently less favorable with approximately 33-75% of individuals becoming seizure free. The relative poor prognosis can be explained by that FCD is often invisible on MRI and it’s more difficult to define the epileptogenic zone, so we have to depend on demiology, EEG or functional neuroimaging. The other factor affecting the relative poor surgical outcome is that even after removal of all visible lesion on MRI, residual microscopic lesions can still be epileptogenic. There are evidences that indicates that even patients with MRI abnormalities who have respective epilepsy surgery for FCD have worse surgical outcomes than those patients who have surgery for other focal lesional epilepsy syndromes.
In a meta-analysis made by Rowland et al about possible predictor of seizure freedom after surgical treatment of FCD they analyze two thousand and fourteen patients from 37 studies published. From them the overall rate of seizure freedom in Engel Class I after surgery was 55.8% +/- 16,2%. They determine that partial seizures, detection with MRI and type II Palmini histological classification were associated with higher rates of postoperative seizure control. As a treatment related factor, complete resection of the anatomical or electrographic abnormality was the most important predictor overall of seizure freedom. These authors conclude that neither age nor electroencephalographic location of the ictal onset significantly affected seizure freedom after the surgery.
In this chart we can see the strong relation between the surgical outcome and the complete resection, seeing that the seizure free is much more frequent in those patients with complete resection. According to this, Cohen-Gadol et al published a serie of 22 cases in which they demonstrated that the histological evidence clear margins was significantly associated with an improved seizure outcome (p<0,003)
Conclusions
• FCD etiology is yet unknown but genetic an environmental factors are meant to be the cause.
• MRI, EEG, PET, SPETC and SEEG must be studied when we face a patient with FCD.
• Seizures as a result of FCD are more difficult to control after surgery even if we can identify lesions on the MRI.
• The most important factor for seizure free in FCD surgery is the complete resection.

Muy bueno, me ayudo bastante