PROPOSALS AND NUANCES TO AMELIORATE THE SURGICAL RESULTS OF TEMPORAL LOBE EPILEPSY
Rafael García de Sola
Catedrático y Jefe de Servicio de Neurocirugía
Hospital de La Princesa
Universidad Autónoma de MadridInvitación a participar en la Mesa Redonda sobre Epilepsy Surgery.
European Association of Neurosurgical Societies Meeting. Madrid, 19-21 de Octubre de 2015.
Reproducción de la conferencia
Introduction
Good morning, everyone
On behalf of the team of Hospital de La Princesa, I would like to thank the EANS Meeting Organization Committee for inviting me to participate in this Round Table.
My aim is to talk about certain proposals and nuances, that could change our strategy in epilepsy surgery in order to improve the surgical results.
Let me introduce myself
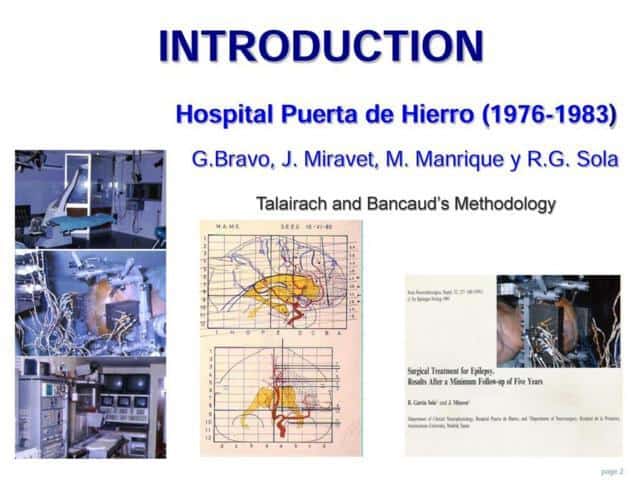
The first Epilepsy Surgery Program in Spain was created in 1976, in Hospital Puerta de Hierro, following Tallairach and Bancaud’s methodology.
I was in charge of this program from 1978 to 1983
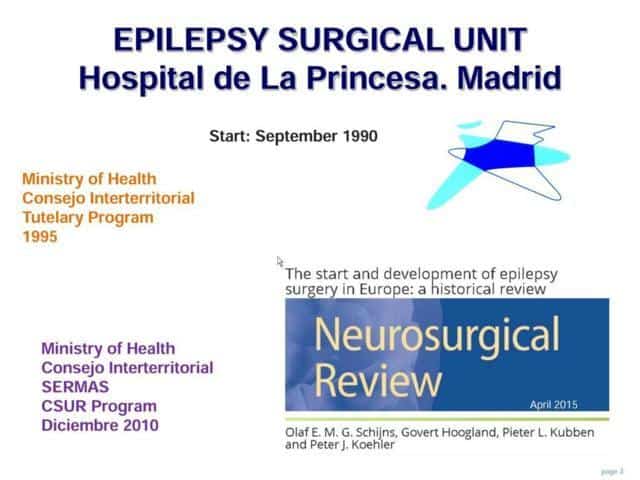
I moved to Hospital de la Princesa, as Head of Department, in 1985. Today, just 30 years ago.
In 1990 we began an Epilepsy Surgery Program that has been approved by the Ministry of Health, in 1995 and confirmed in 2010, as a National Reference Centre for this pathology
Methodology
Going forward, firstly, I will briefly explain you our methodology
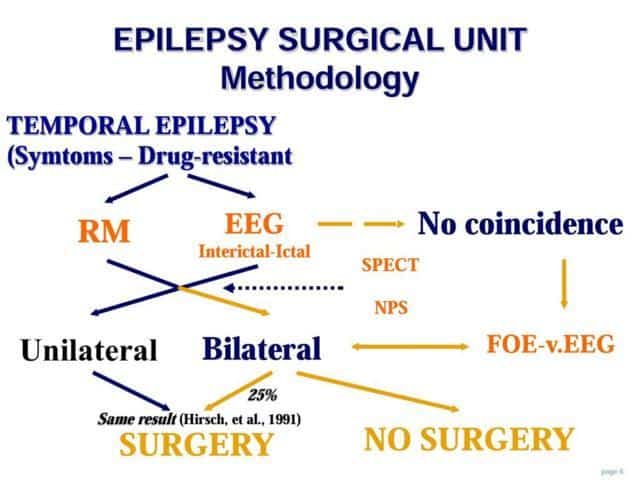
The first step is the selection of patients and the non-invasive studies
As you can observe in this flow-chart, we study the patient with MRI, EEG, SPECT and Neuropsicological evaluation.
If there is a clear coincidence and unilateral focus, we could go directly to surgery
If some discrepancies appear, or there are signs of bilaterality or doubt of extratemporal implications; we prefer to explore the patient with foramen ovale electrodes or other kind of intracranial electrodes.
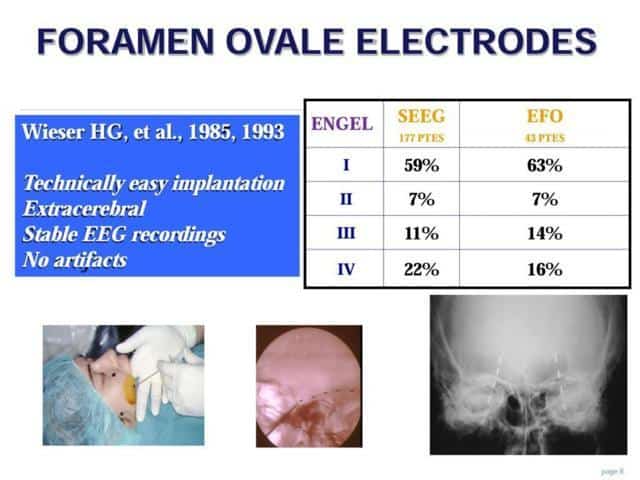
In this phase of Invasive Studies, I would like to emphasize the usefulness of foramen ovale electrodes
These were proposed by Wieser in 1985.
They are technically easily implantable
They are located extracerebral and the EEG recordings have no artifacts and are very stable
He explained that the results were similar or even a bit better than the surgical results after a SEEG study with depth electrodes
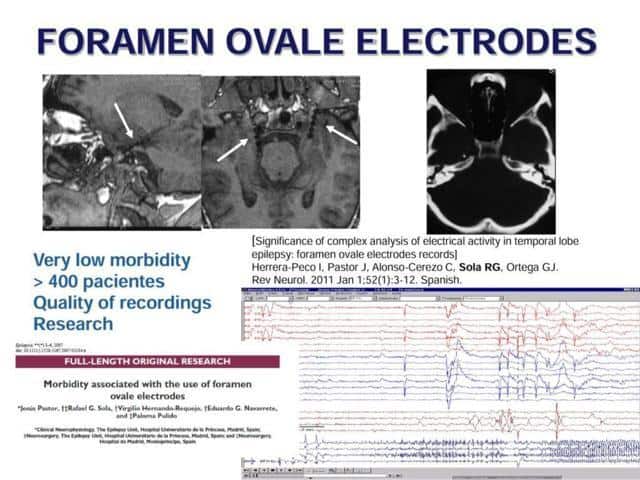
We are fond of this FOE exploration
We have a wide experience with this, with low morbidity, a good quality of recordings and they have served us as a good base to run lines of research
Once we have clearly located the epileptogenic zone to be excised, we operated on the patient.
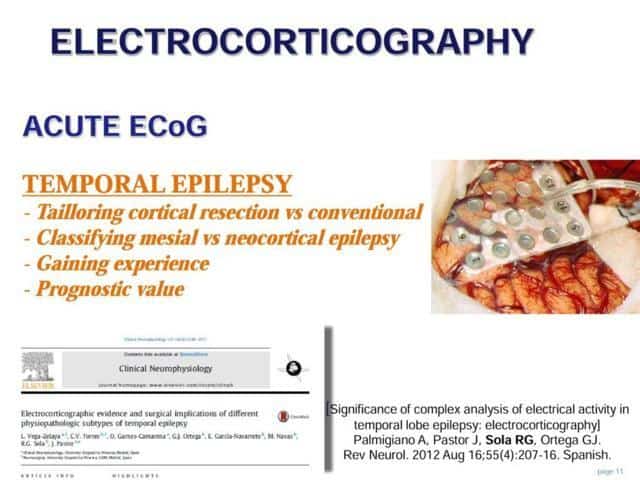
As a routine, we perform an electrocorticographic exploration
The idea is to carry out a tailored cortical resection
Besides, the ECoG could help us to classify the kind of temporal lobe epilepsy, to give us a prognostic value, and to maintain a way of getting experience.
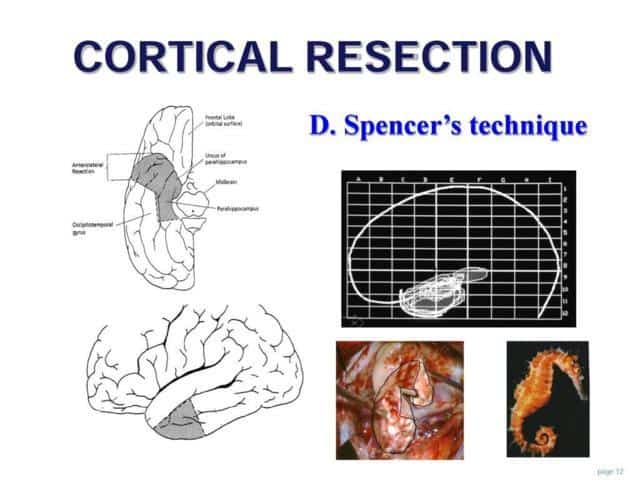
The cortical resection is made following the Spencer’s technique, with a fist step of anterior neocortical removal, following by the amigdalohipocampectomy “in block”.
Regarding the surgical results,
Results
I would like to draw your attention to some nuances
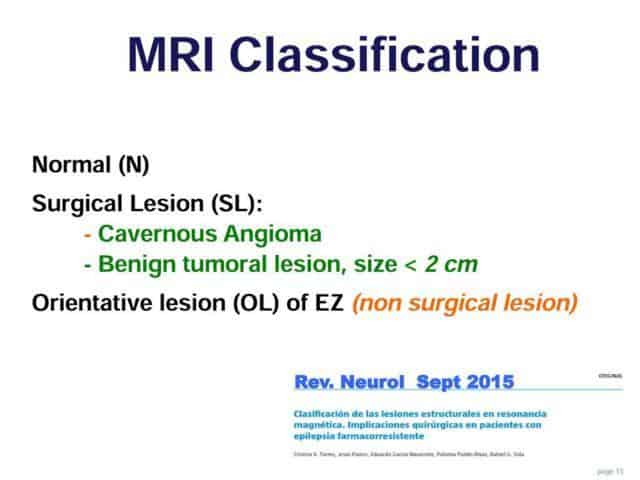
Looking at the MRI, we have preferred to classify the structural lesions in two subgroups:
Surgical lesions, as cavernous angioma and benign tumors are
Orientative lesions. These are all the other type of lesions, including mesial sclerosis or dysplasia, that don’t have surgical indications. Except if we demonstrated that they are in straight relationship with the epileptogenic zone. But they are going to help us to find it
The third category is the group of normal MRI
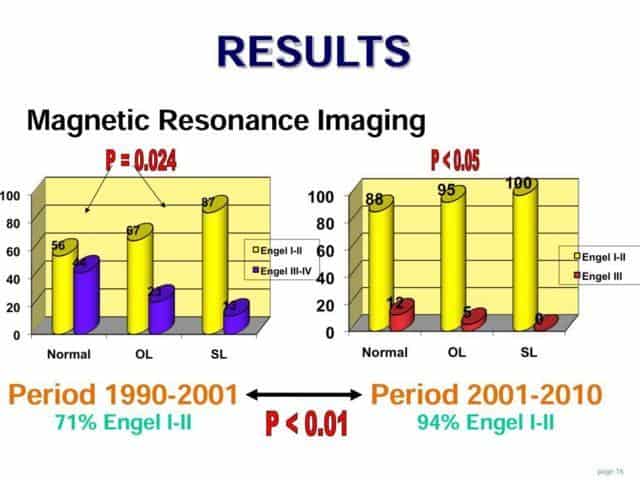
In this slide I would like to present our experience, divided in two period of ten years each.
It is relevant that there are statistically significant differences between the described MRI groups.
The best results are obtained with the surgical lesions, following by the orientative lesions
The group of patients with normal MRI has worse results. However, with experience, we have decreased this difference. Improving the results in normal MRI from 56% to 88% of Engel I-II
Proposals and nuances
Based on these results, I would dare to put forward certain proposals or nuances
If we take a closer look at the MRI findings, there are authors who question whether to accept patients with normal MRI to a surgical program or not
On the other hand, there are authors who get good results.
But they make use of other images tests and invasive studies
We agree with the latter ones.
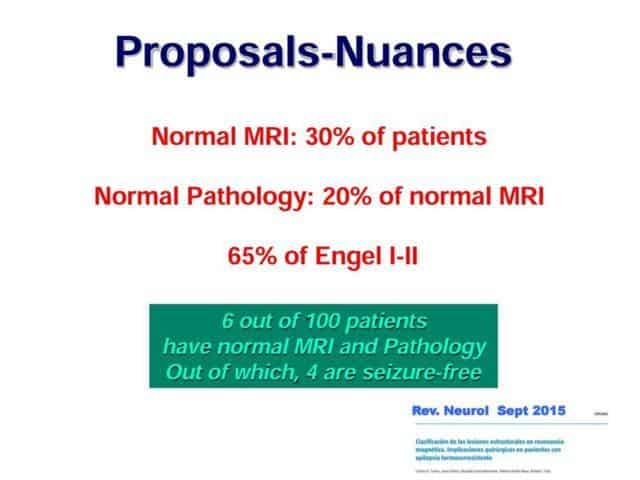
Moreover, we have found patients with normal MRI and normal Pathology.
According to our results, 30% of patients have had normal MRI. Out of which, 20% don’t have abnormal structure in conventional pathological studies.
But, although both MRI and pathology have been normal, we have obtained a 65 % of seizure-free patients
Then, we emphasize that no patient should be excluded of an epilepsy surgery program because of normal MRI
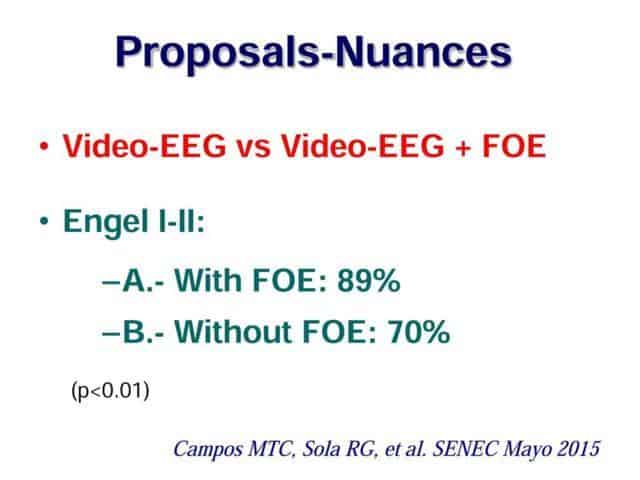
We have recently presented our results, comparing a group of temporal lobe epileptic patients previously explored with Video-EEG alone o with Foramen ovale electrodes.
The group explored with foramen ovale electrodes was larger than the group without this semi-invasive exploration
And the results show almost 20 points more in the percentage of good results.
Although the group of simple Video-EEG included easier patients
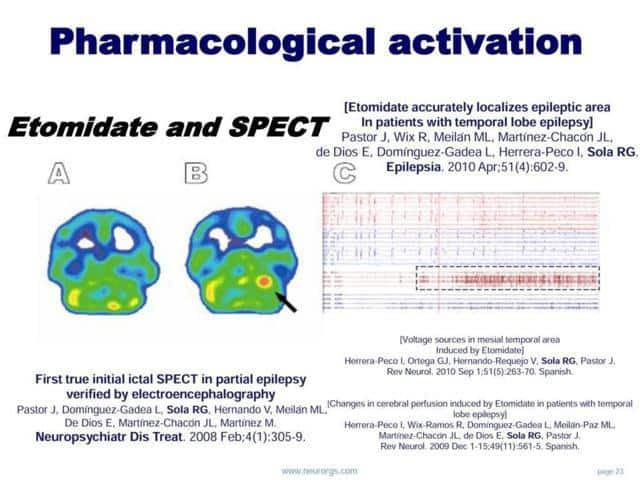
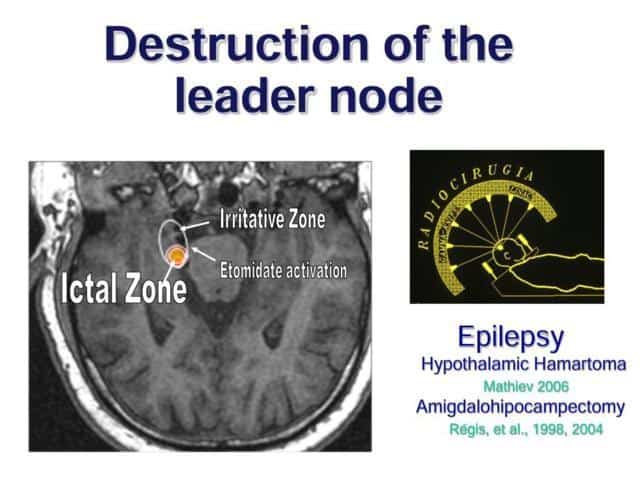
Another nuance that I would like to present, is the possibility of helping us with pharmacological activation, to define the epileptogenic zone
This action has been profited by us, administering simultaneously the isotope. With the idea of performing a pharmacological ictal SPECT
In the same way, we use as a routine Etomidate during ECoG exploration, to clarify the irritative epileptogenic zone
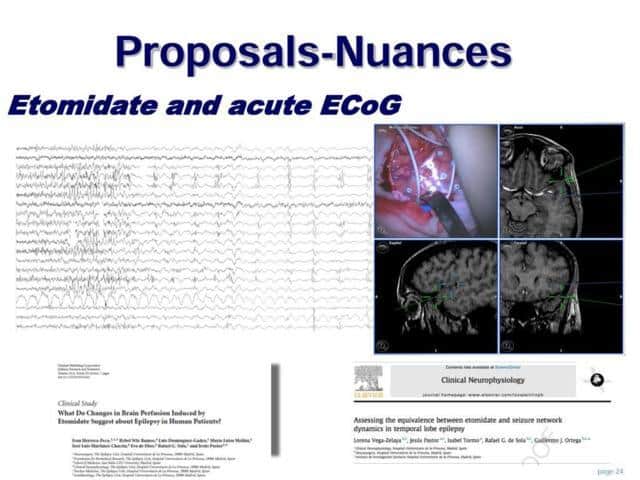
Besides, we have analyzed in an out-line process, the ECoG signals. Demonstrating that certain synchronization process exists
Moreover, we have found that cortical activity works as a network with different kind of nodes.
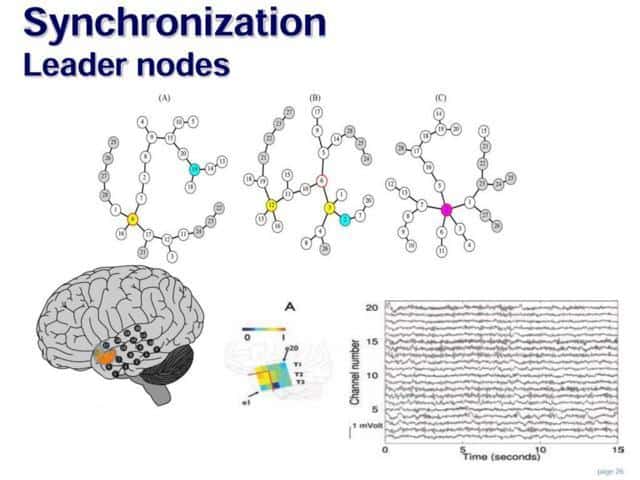
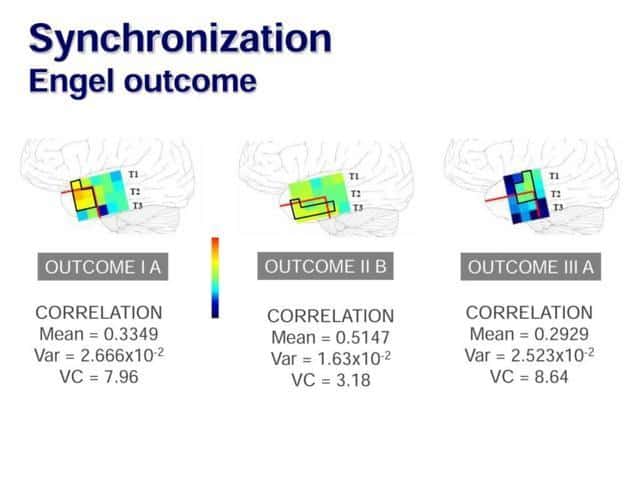
And, interestingly, there is a difference between patients to whom we have removed determined nodes of this network or not
Therefore, it seems that resection of sharply defined clusters in the lateral cortex of patients with mesial temporal lobe epilepsy could be important for functional outcome
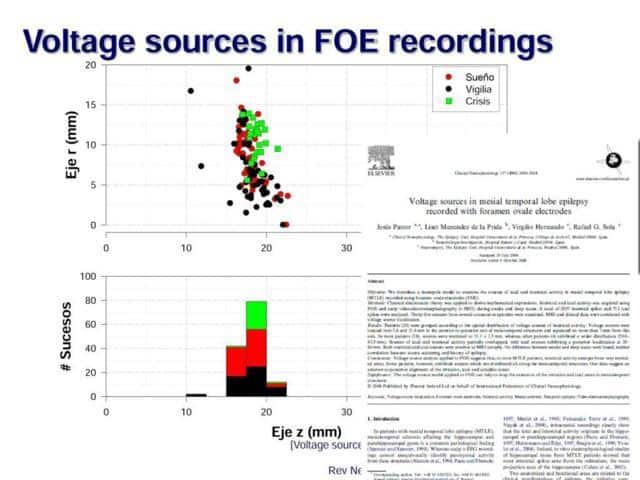
Finally, we have studied and explored the voltage sources that produces the signal recorded by foramen ovale electrodes
An important finding was that certain patients, with normal MRI, Normal IQ and normal memory, presented a very clear zone of ictal onset (in one or two contacts)
These patients have no surgical indication, because of the postoperative neuropsychological deficits.
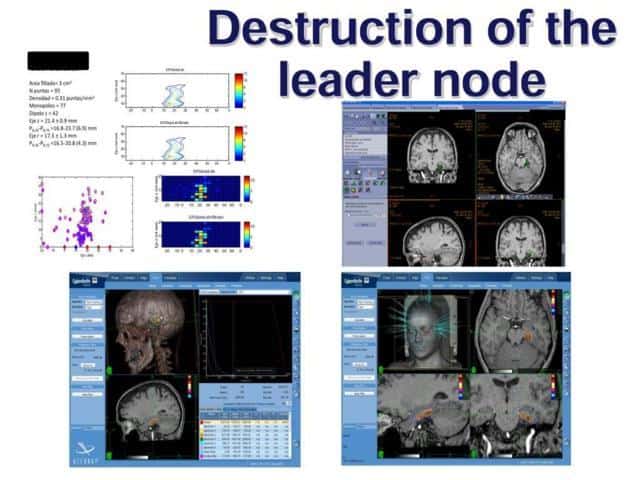
As this ictal zone is a very circumscribed and small region, we have proposed to performed a small radiosurgical lesion
It is a research project that has been admitted by the Ethical Committee and FIS, one of our National Research Agencies
Until now, we have treated 3 patients and we are waiting for the results
Conclusion
In conclusion:
In non-lesional MRI patients we could get more than 80% of good results
Taking this into account, the number of patients to be involved in an epilepsy surgery program might be increased
We propose Foramen ovale electrodes as a semi-invasive exploration
As well as pharmacological activation and the possibility of performing pseudoictal SPECT in doubtful cases
In lesional temporal epilepsy the good surgical results are higuer than 90%
And, again, the foramen ovale electrodes exploration could be very useful in cases with orientative lesion in MRI
We have to be ready to accept the new concepts of networks in epilepsy.
And the possibility of having different subtypes in temporal lobe epilepsies
Consequently, do we have to take into account the leader nodes in cortical resection?
Could we open a new way of treatment of patients with normal MRI, normal IQ and normal memory?
Designing a small lesion based on the voltage sources found in the foramen electrodes exploration. This could be performed by means of radiosurgery or other tools
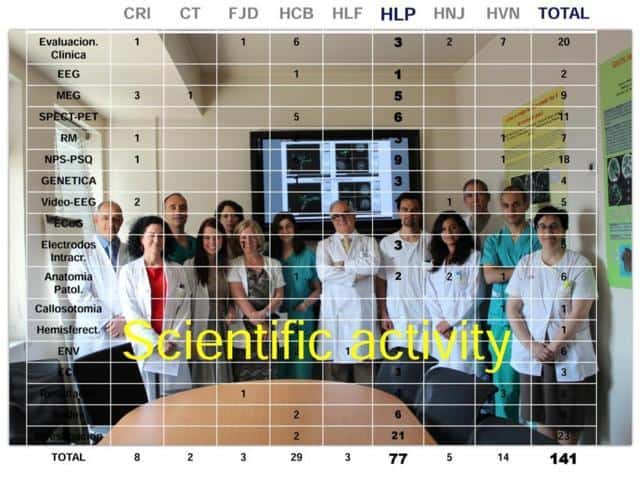
I have to thank each one of my team for their collaboration. They have produced more than half of scientific contribution in Spain to the epilepsy surgery field.
THAN YOU very much for your attention