Conferencia sobre Estimulación Cerebral Profunda – DBS
Brain & Chip ’24: University Miguel Hernandez – Alicante, España
Conferencia del Dr. Rafael García de Sola como invitado a participar en el BRAIN&CHIP ’24: 2nd INTERNATIONAL CONGRESS ON NEURAL ENGINEERING, ARTIFICIAL VISION, AND INTRACORTICAL BRAIN COMPUTER INTERFACES.
Celebrado en Elche (España) los días 11, 12 y 13 de Noviembre 2024.
El principal objetivo de la reunión The Brain and The Chip 2024 es proporcionar un foro global para debates amplios y centrados entre los líderes en el desarrollo de interfaces neuronales intracorticales. Se pretende reunir a investigadores de renombre, clínicos y expertos en diversos campos -ingeniería neuronal, interfaces cerebro-ordenador intracorticales, microelectrónica, visión artificial, neurocirugía, neurología, ciencia de los materiales, IA inspirada en neuronas, etc.- para fomentar colaboraciones, intercambiar conocimientos y explorar avances en interfaces intracorticales.
11 de Noviembre de 2024. Universidad Miguel Hernández. Elche. Alicante.
Seguir la presentación completa: Sobre Estimulación cerebral profunda – DBS
Resumen de la conferencia
Este documento proporciona una visión completa del impacto de la estimulación cerebral profunda (DBS) en la Neurocirugía moderna, destacando sus aplicaciones clínicas, metodología y resultados.
La estimulación cerebral profunda (DBS -Deep Brain Stimulation-, por sus siglas en inglés), es una técnica avanzada de Neurocirugía Funcional utilizada para tratar trastornos neurológicos y psiquiátricos resistentes a otros tratamientos. A continuación, se resume el contenido principal:
Objetivo de la neurocirugía funcional:
- Restaurar o equilibrar funciones alteradas del cerebro mediante estimulación o inhibición.
- Aplicaciones en:
• Trastornos del movimiento (como el Parkinson y la distonía).
• Epilepsia farmacorresistente.
• Dolor crónico.
• Trastornos psiquiátricos severos.

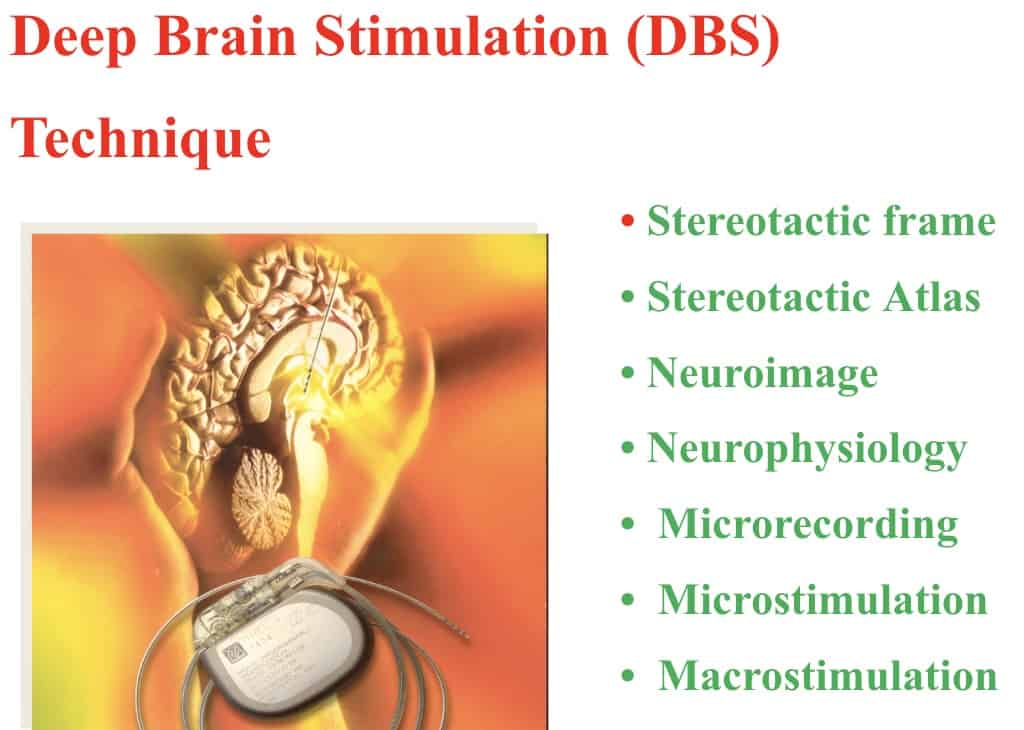
Técnica de estimulación cerebral profunda (DBS):
- Principios básicos:
• Implante de electrodos en regiones específicas del cerebro para transmitir impulsos eléctricos de alta frecuencia.
• Uso de imágenes y herramientas estereotácticas para localizar con precisión los objetivos quirúrgicos. - Ventajas frente a técnicas ablativas:
• Reversibilidad y posibilidad de ajuste.
• Mayor complejidad y coste, pero menor invasividad permanente. - Regiones objetivo:
• Núcleo subtalámico, globo pálido y núcleo centromediano para trastornos del movimiento y epilepsia.
• Hipotálamo y cíngulo subgenual para trastornos psiquiátricos (como depresión resistente). - Beneficios observados:
• Mejoras en síntomas como temblores, rigidez, bradicinesia, y epilepsia resistente.
• Control de comportamientos agresivos y depresión en casos extremos.
Aplicaciones clínicas destacadas:
-
• Trastornos del movimiento:
• Parkinson: mejora de síntomas motores y reducción de efectos secundarios de medicamentos.
• Temblor esencial y distonía: reducción significativa de los síntomas.
• Epilepsia:
• Estimulación del núcleo centromediano del tálamo y otras regiones específicas.
• Psiquiatría:
• Primera neuroestimulación en España para agresividad resistente.
• Casos documentados en depresión bipolar y trastornos obsesivo-compulsivos.
• Dolor crónico:
• Estimulación para tratar dolor neuropático y resistente a medicamentos.
Metodología avanzada:
-
• Planificación quirúrgica: uso de neuroimagen, atlas estereotácticos y registro neurofisiológico.
• Estudios intraoperatorios: registros eléctricos para confirmar ubicación y respuesta.
Conferencia sobre Estimulación cerebral profunda – DBS
Good morning,
First of all, I would like to thank the organizers of this Meeting, for inviting me to participate.
This talk will focus on my own experience with deep brain stimulation, within the field of neuromodulation.
Firstly, I’d like to begin by talking about Functional Neurosurgery.
Then, I will focus on lesional surgery and, finally, on neuromodulation.
Functional Neurosurgery is basically surgical procedures that are aimed at modifying and altering brain functions.
There are 4 classic groups of diseases that are addressed in this subspecialty.
Psychotic disorders, movement disorders, epilepsy and pain.
The aim is for the patient to recover to a state that is as close to normal as possible.
Thus, surgical treatment is aimed at injuring or inhibiting excitatory centers.
Or, in the opposite way, stimulating inhibitory centers.
Restoring a certain balance similar to normal.
But, as it has been shown in this Meeting, new possibilities of neuromodulation are opening up.
As a result, Functional Neurosurgeons are now collaborating with Basic Sciences and Engineering experts, to improve brain function.
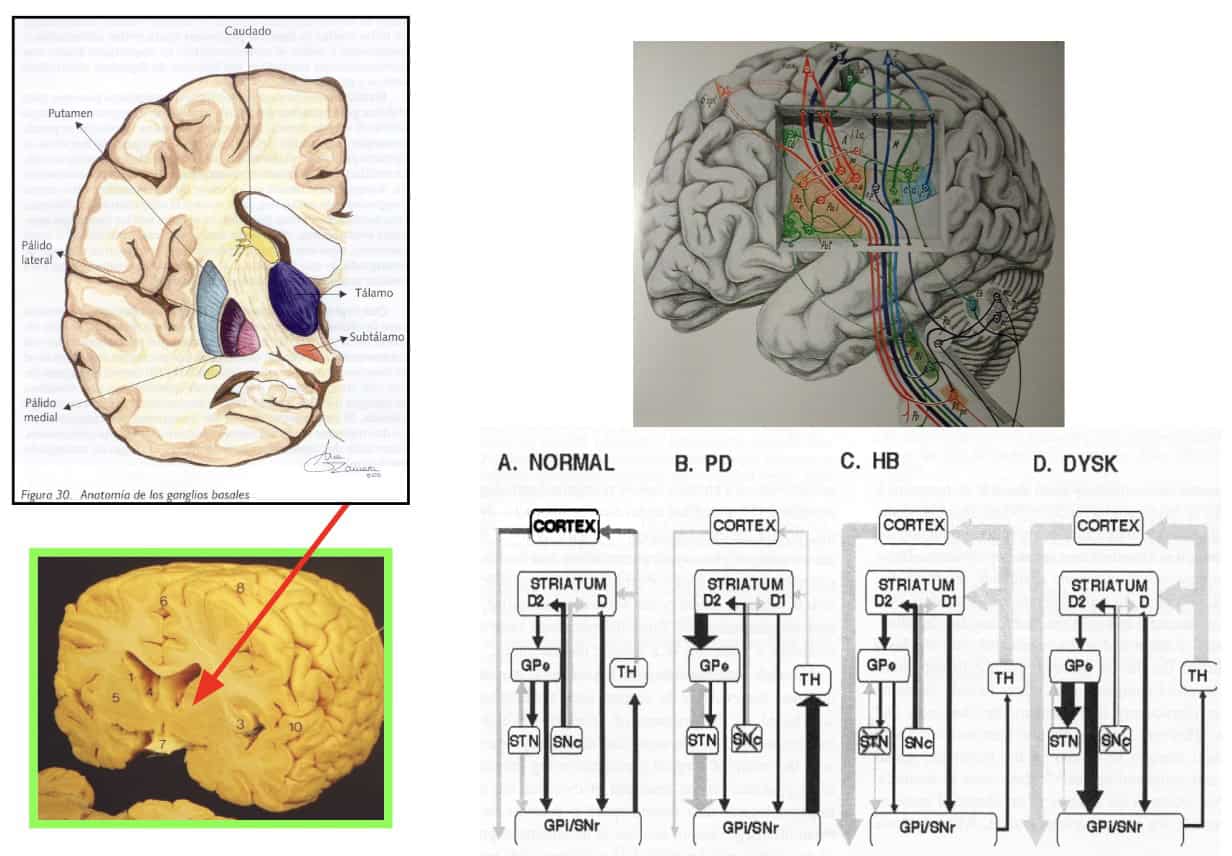
Coming back to the classic model of Functional Neurosurgery, the first step has been to know the pathophysiology of certain diseases.
If we take movement disorders, as an example, we locate and target the nuclei where we achieve a new positive balance for the patient.
But most of these treatments target nuclei located in the subcortical region of the brain.
To reach these nuclei, neurosurgeons have had to design a method or technique.
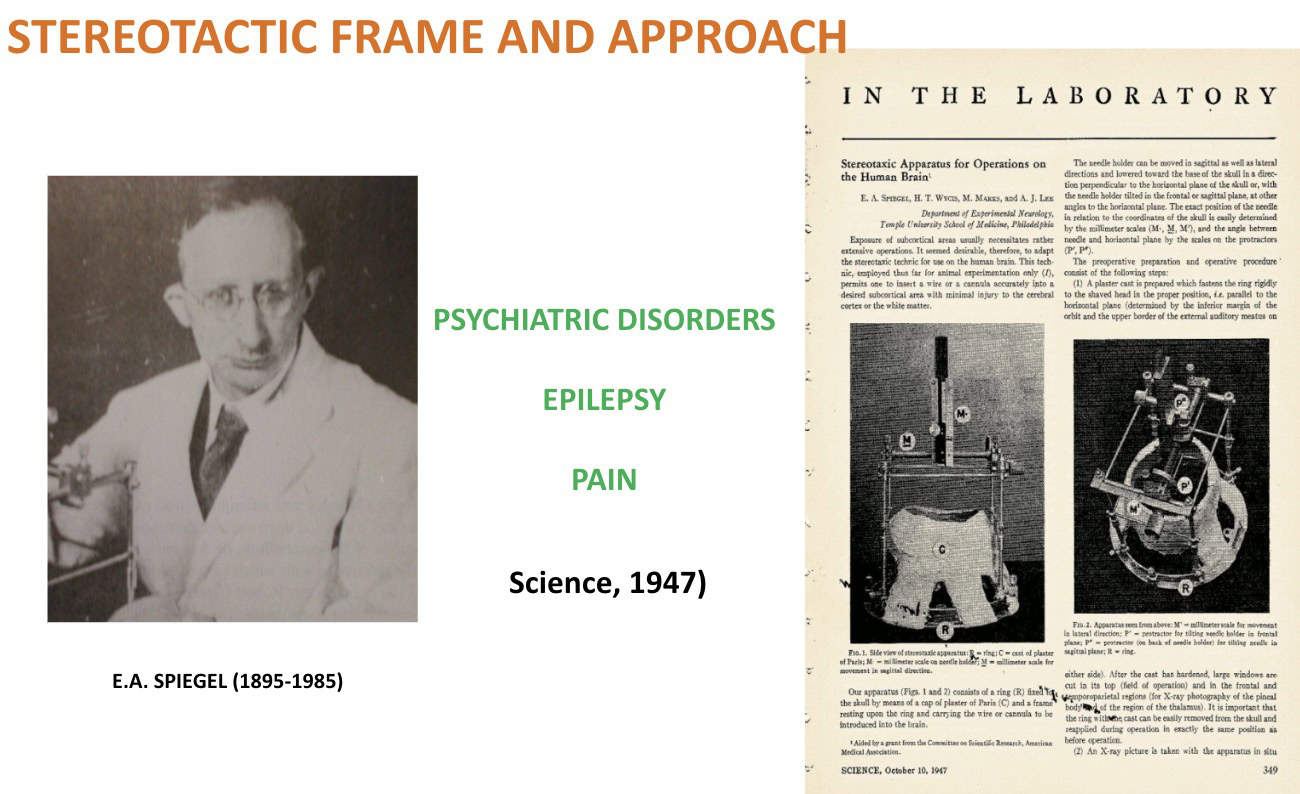
The result was Stereotactic Surgery.
This allowed them to carry the element that stimulates or injures these nuclei, safely, accurately and in a minimally invasive way
The pioneer of this technique was Spiegel who, assisted by the engineer Wycis, carried out the first operation in 1947.
They applied this surgical approach to the treatment of psychiatric pathologies, epilepsy and pain.
Which, in those years, had no possibility of effective treatment.
Not even with medication.
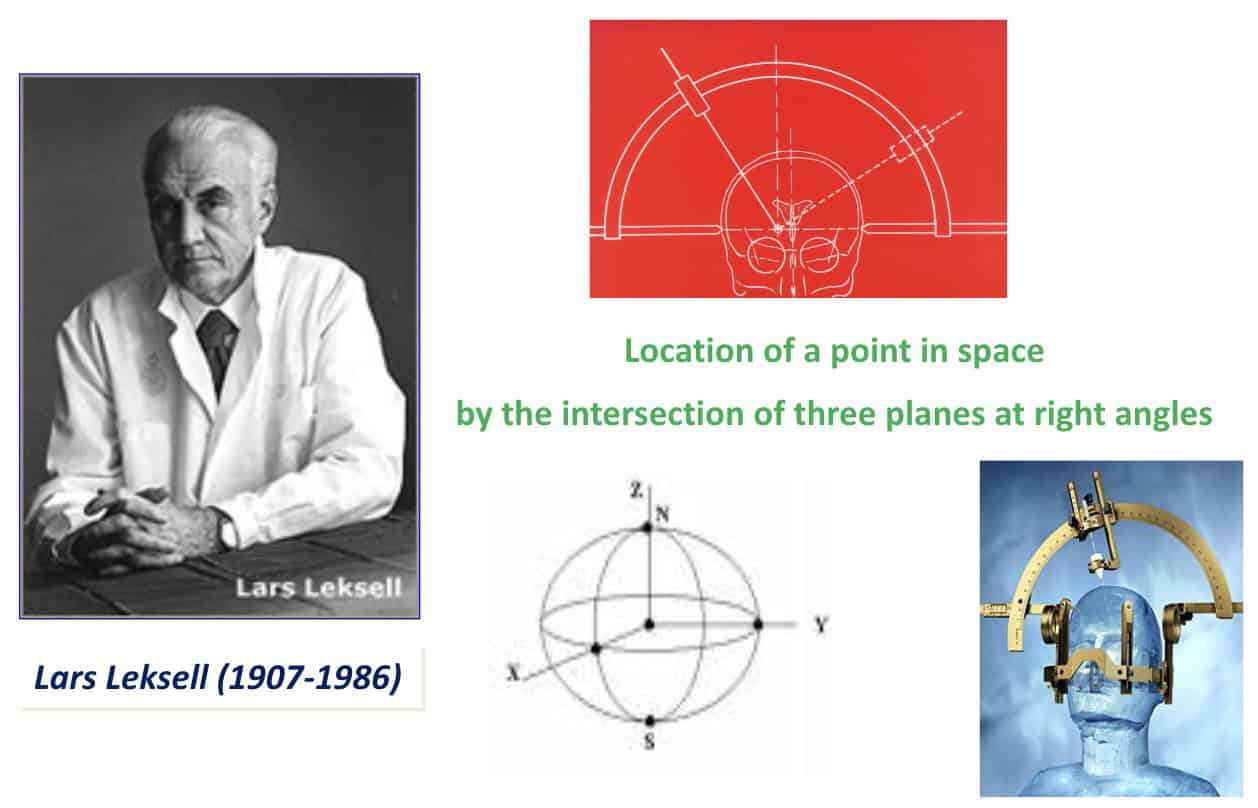
The stereotactic guide or frame was perfected by Leksell.
His design is the most widely used nowadays.
In this area, stereotactic frames are used for:
- – One, surgical approaches that allow for the introduction of special cannulas to take biopsies.
– Two, to support instruments such as the palidotome, to mechanically injure a nucleus.
– And three, to carry an electrode that allows stimulation, knowing the function, and then performing a thermal lesion.
Nowadays with radiosurgery or high intensity ultrasound, directed stereotactically, it is possible to generate a lesion in a totally non-invasive way.
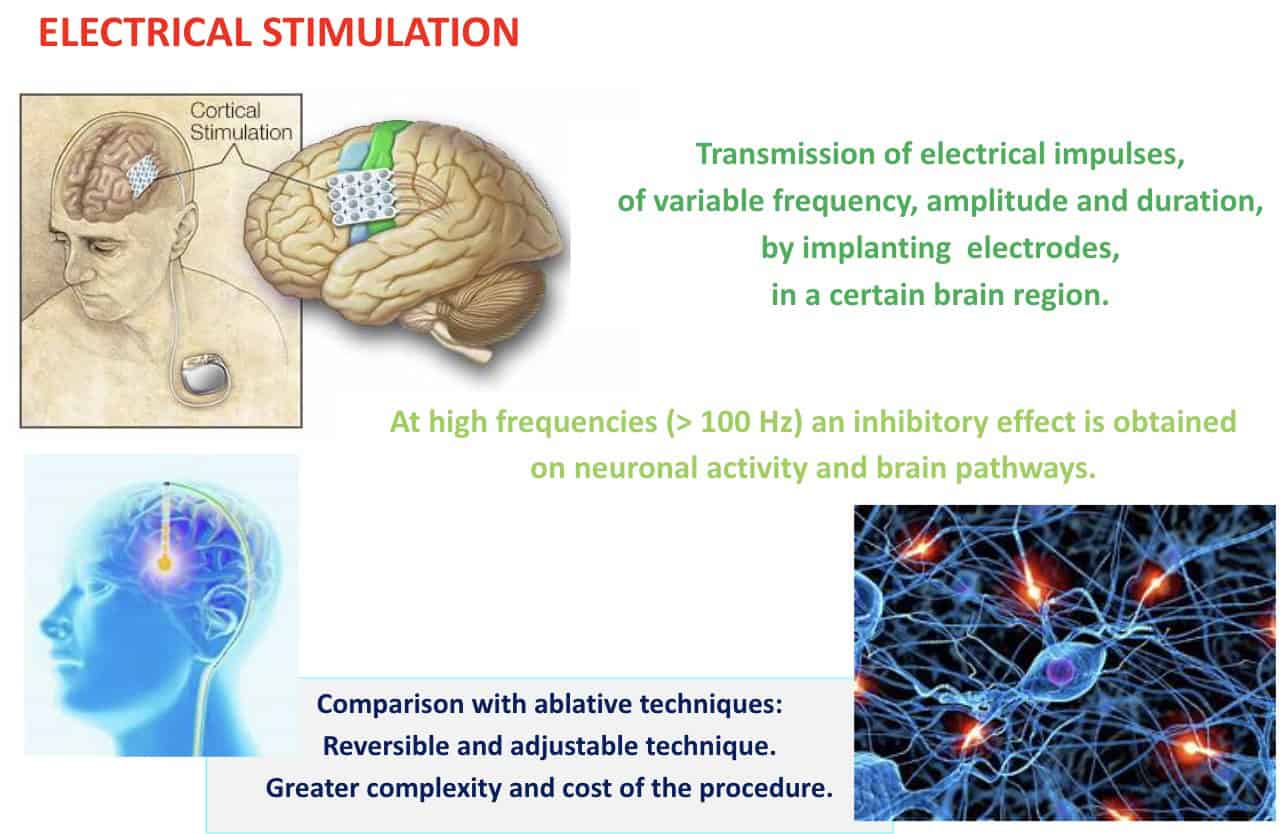
The other, increasingly important area in Functional Neurosurgery is electrical stimulation.
This is done by implanting cortical or subcortical electrodes, to inhibit exaggerated functions or generate useful neuronal activity.
This neuromodulatory method can be used in deep subcortical areas.
Hence the name “deep brain stimulation”.
To carry out this complex treatment, several elements are required, which you can see here and that we will discuss later.
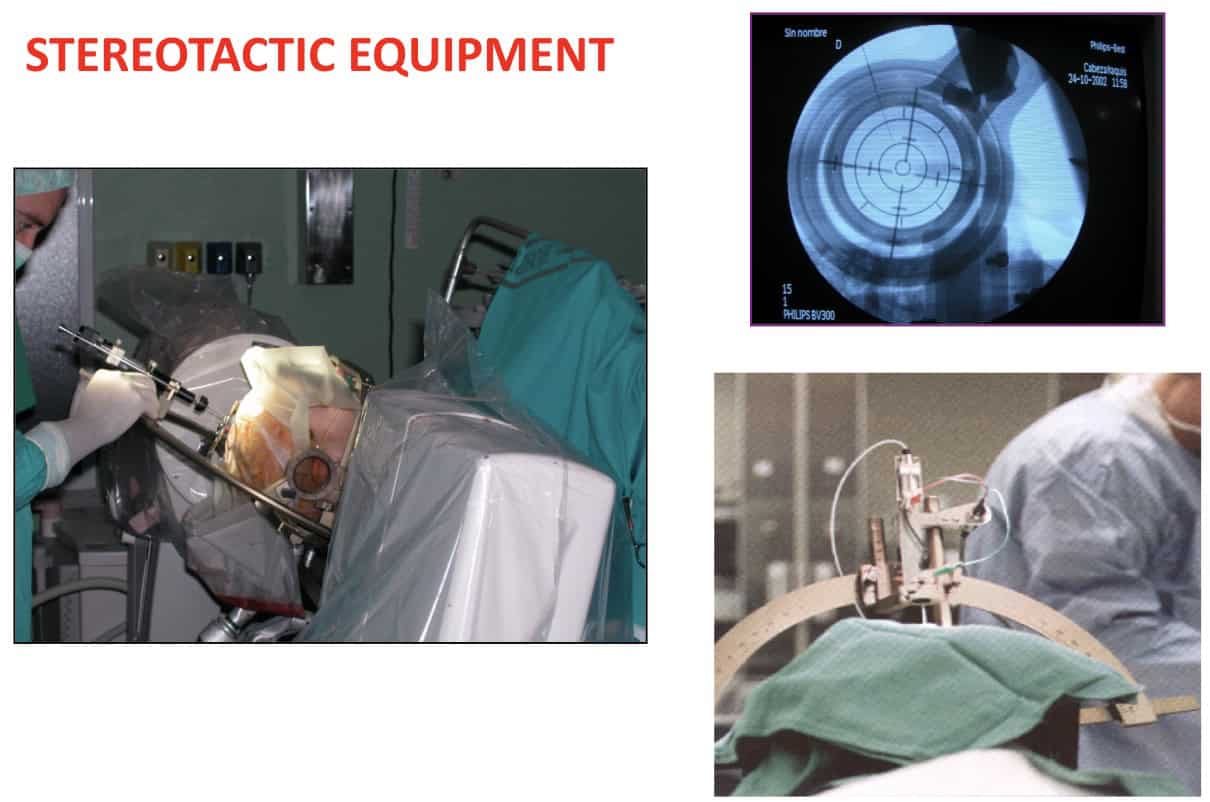
Let’s look at the equipment needed.
Firstly, a stereotactic guide, such as the one developed by Leksell., is widely used in operating rooms.
This must be complemented with a control X-ray C-arm.
The frame supports the electrode, placed on a micromanipulator, which allows movements of less than 1 mm.
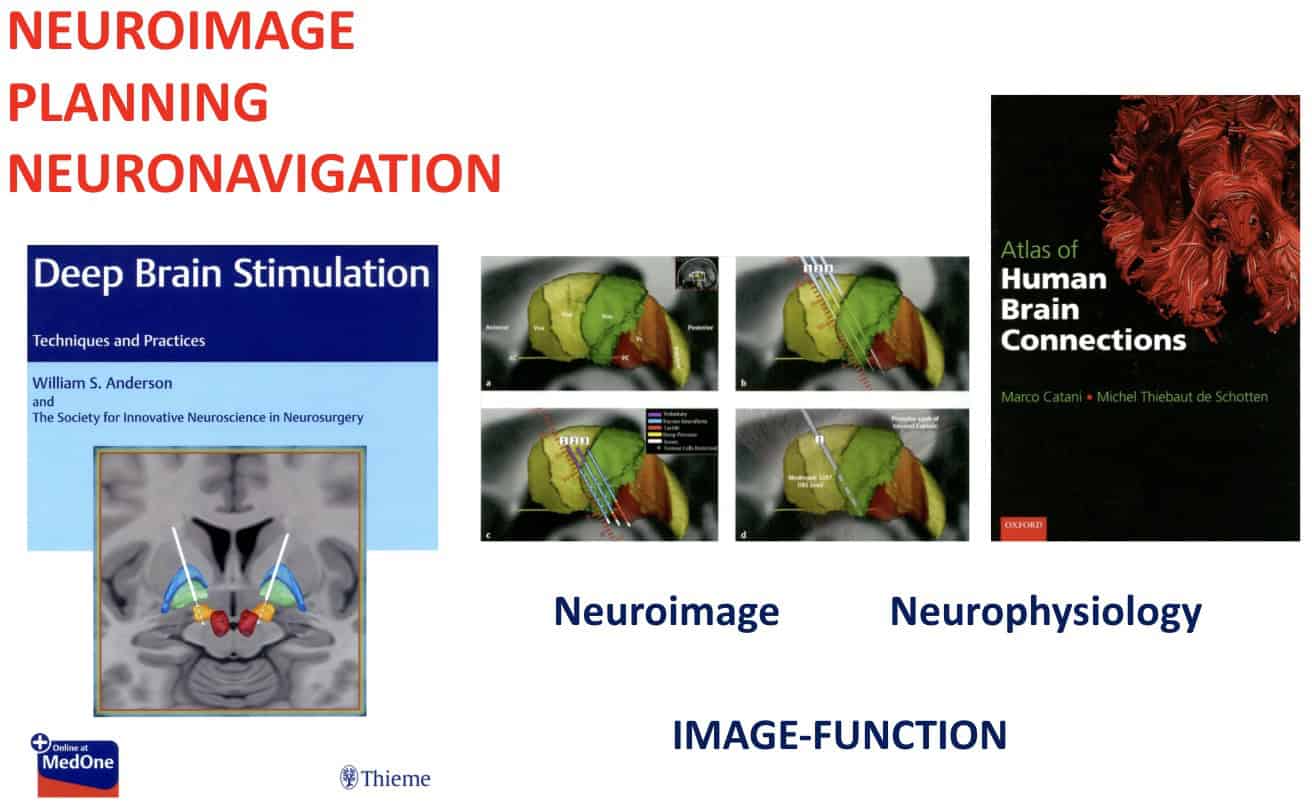
But to reach the desired nuclei, it is necessary to rely on a Stereotactic Atlas.
There are numerous atlases that are based on several anatomical features.
Talairach devised the intercommissural line, that demonstrated a proportionality between the different thalamic and subthalamic nuclei.
Another is the Schaltenbrand Atlas, that gives us the 3D anatomical location of the different nuclei, related to this intercommisural line.
And besides these two, there are several other atlases that can show us somatotropy in the nuclei, which allows us to fine-tune said targets.
At the beginning of stereotactic surgery, everything described so far allowed neurosurgeons to reach these nuclei with a certain degree of accuracy
Operations were supported by simple X-rays, which provided PA and Lateral images of the cerebral ventricles, which were filled with air or iodine contrast.
Since those days, this method has improved dramatically with the advent of CTscan and MRI.
As well as very precise and safe planning programs.
X-ray equipment continues to be used in the operating room, but only for the safety of placement and repositioning of the electrodes on the target.
Furthermore, the classic atlases I mentioned are being continuously improved.
3D images of the different nuclei and their connecting paths have also improved greatly.
This has led to our neurosurgical team acquiring experience in the location and function of a significant number of nuclei or targets.
Let us now analyze each group of diseases that we routinely treat with DBS.
A.- Movement disorders
First of all, movement disorders.
Such as Parkinson’s disease, tremor or dystonia.
Traditionally, tremor in Parkinson’s disease and essential or cerebellar tremors were treated by lesioning certain thalamic nuclei.
In my special operating room in the former Puerta de Hierro Clinic, dedicated to Epilepsy Surgery, we fused the Cooper-Parera guide with the Talairach Frame.
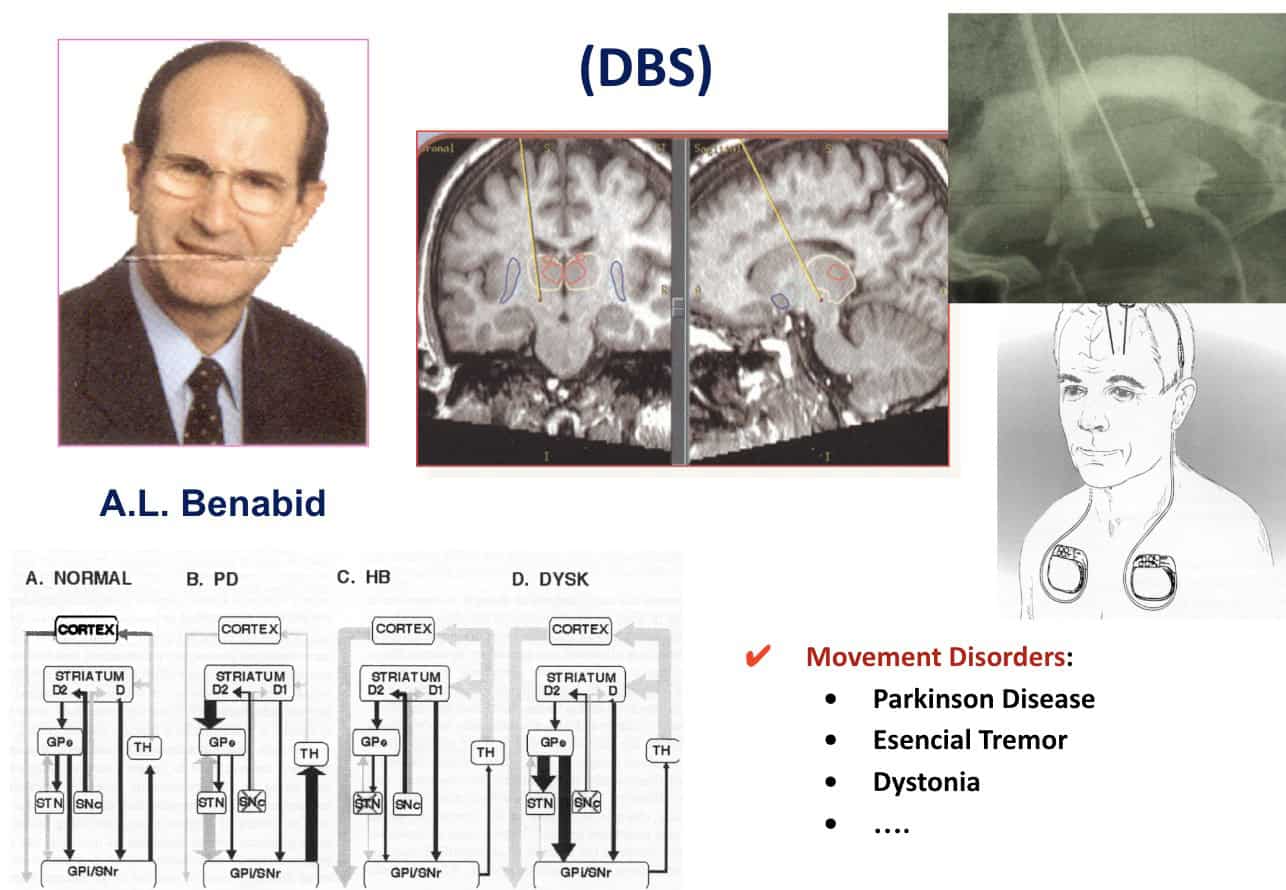
It is thanks to Benabid who, in the 1980s, proposed treating these movement disorders with deep brain stimulation.
Initially at the level of the subthalamic nucleus and, later, when other nuclei were explored, in order to obtain a new balance in the pathophysiological sequence of these diseases.
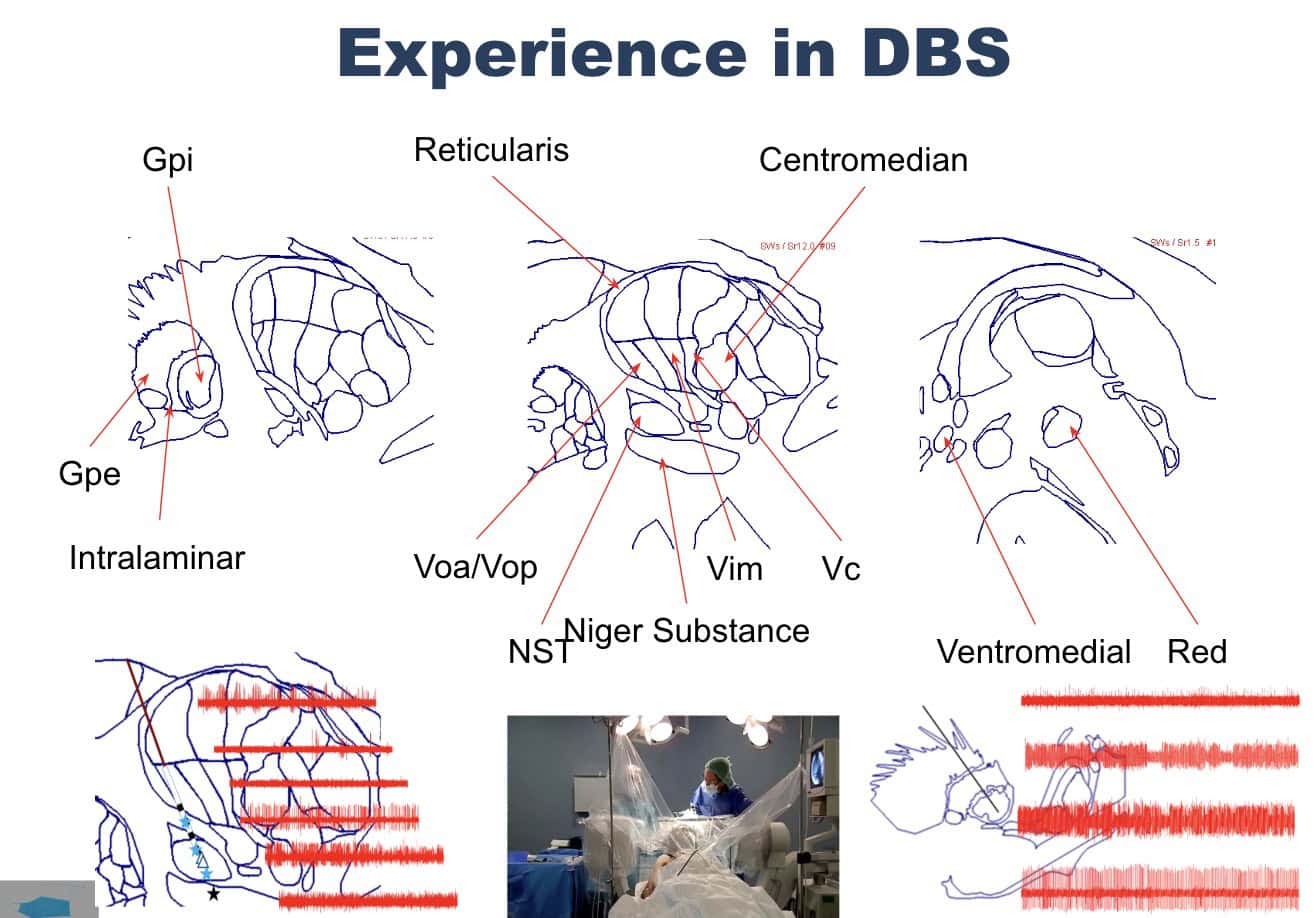
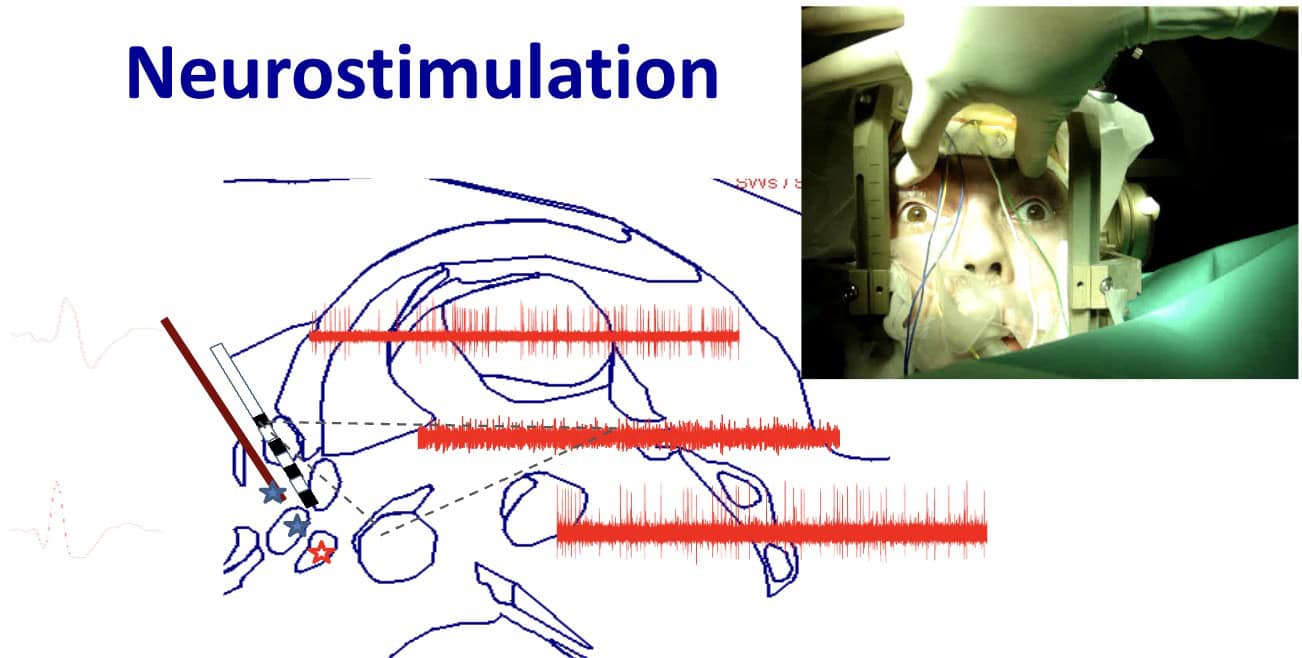
There are two neurophysiological steps in the surgical procedure.
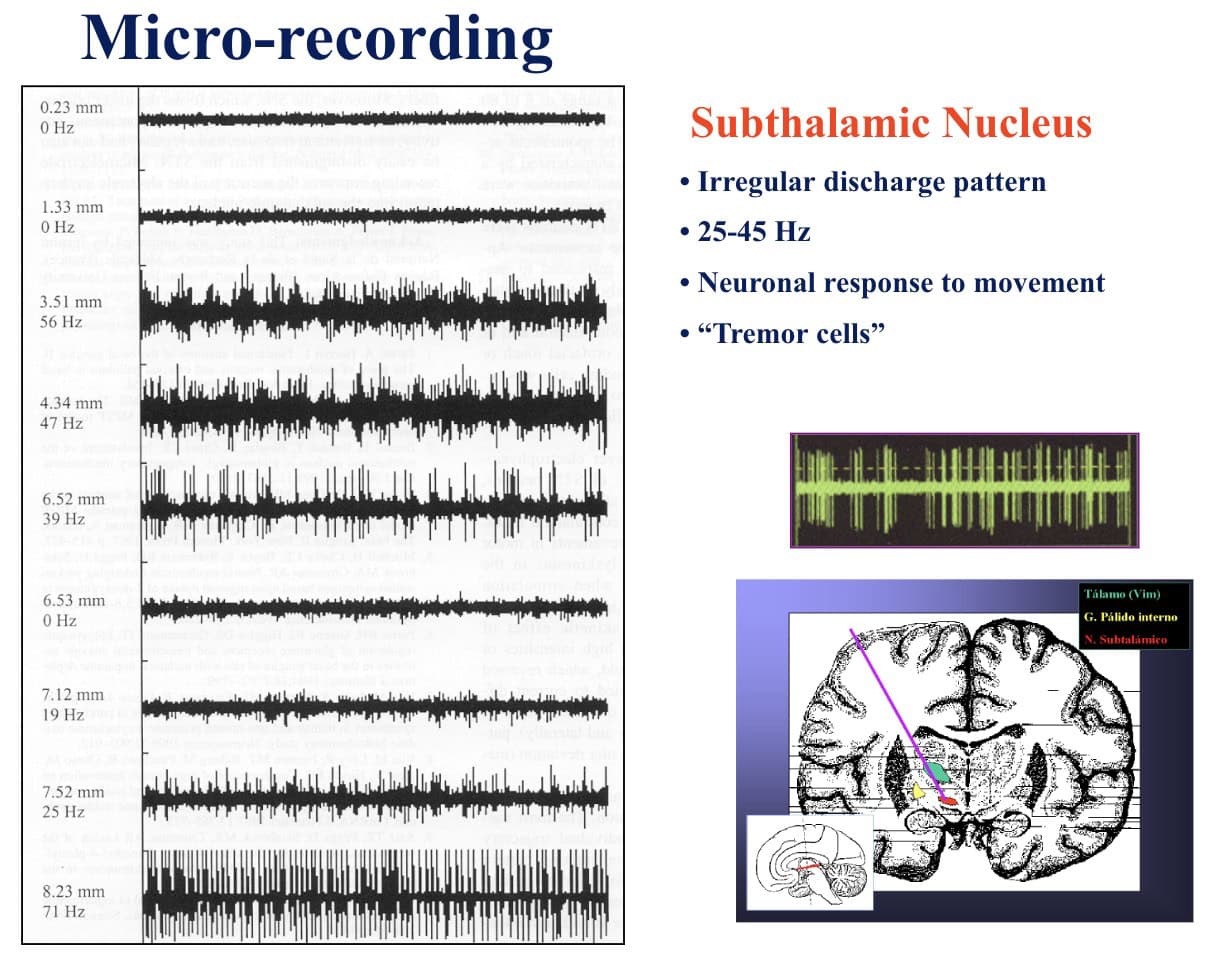
In the first step, microelectrodes are inserted using the micromanipulator.
The neurophysiologist observes the electrical activity of the different neurons corresponding to the nuclei and pathways that are found until we reach the desired target.
In this case, the subthalamic nucleus.
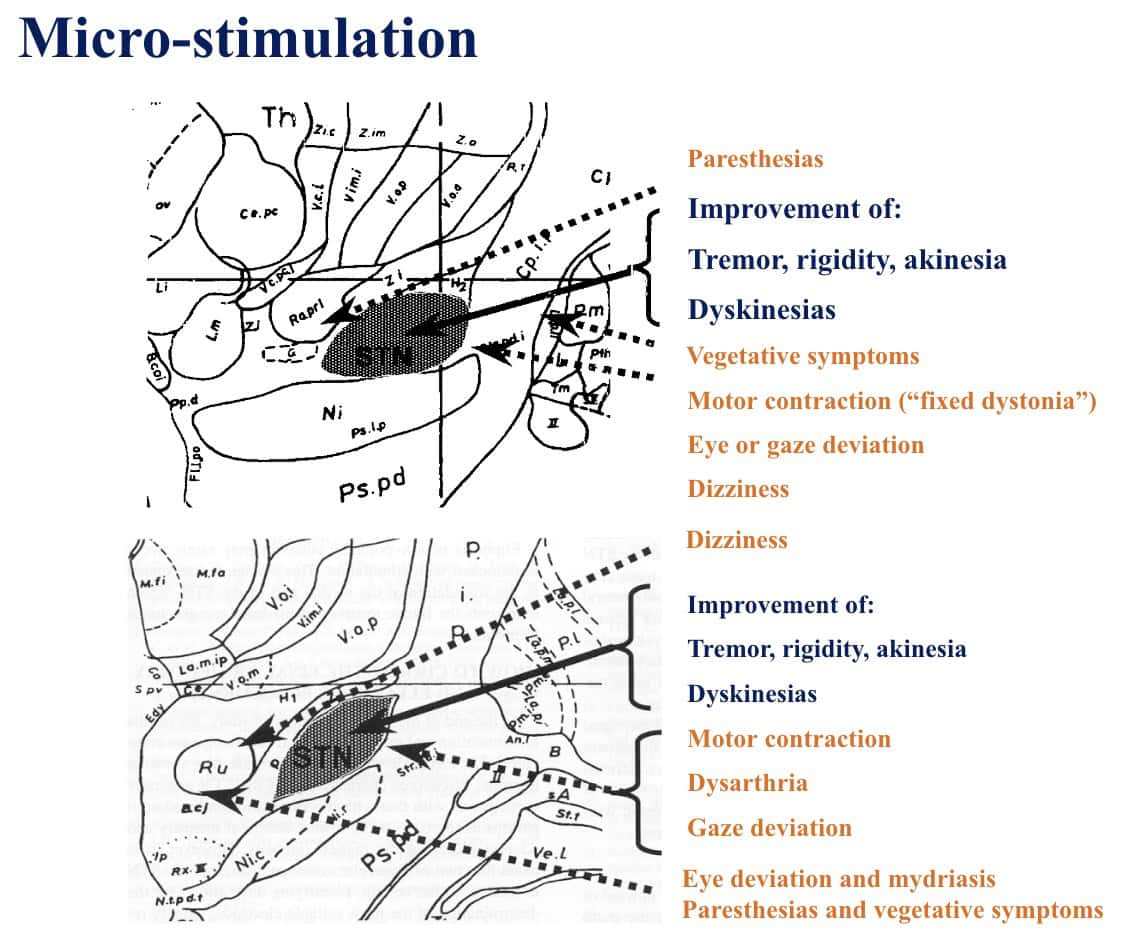
In the second step, stimulation is carried out and patient’s responses are recorded in terms of improvement in tremors, rigidity, etc.
Or, alternately, in adverse effects, in which case, another target must be selected.
This makes it possible to choose the optimal location for the definitve macroelectrode, which is placed after removing the other microelectrodes.
The design of new types of electrodes has improved enormously.
They allow for “directed” stimulation, tailored to the symptoms presented by the patient.
It is more effective and it nullifies any unwanted side effects of stimulation.
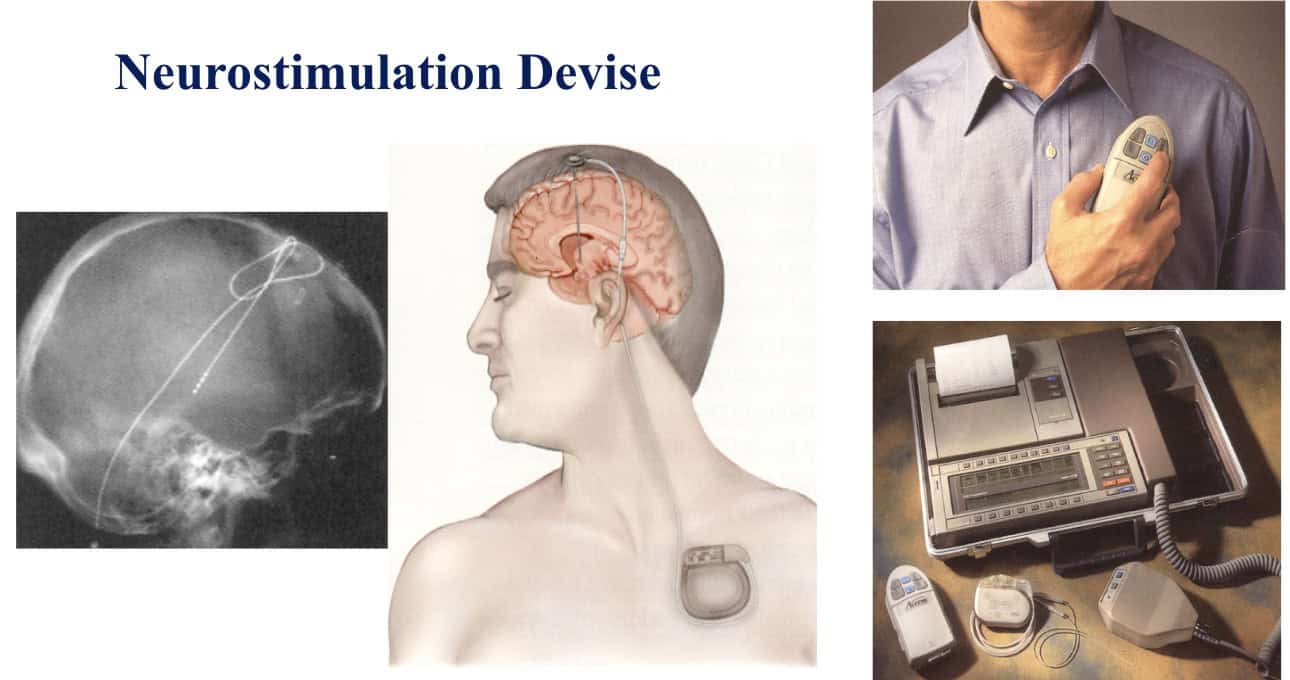
Finally, the macroelectrode is connected to a battery-stimulator, which is placed in a subcutaneous bag.
Later, we modify the stimulation parameters, on an outpatient basis, according to the patient’s clinical response.
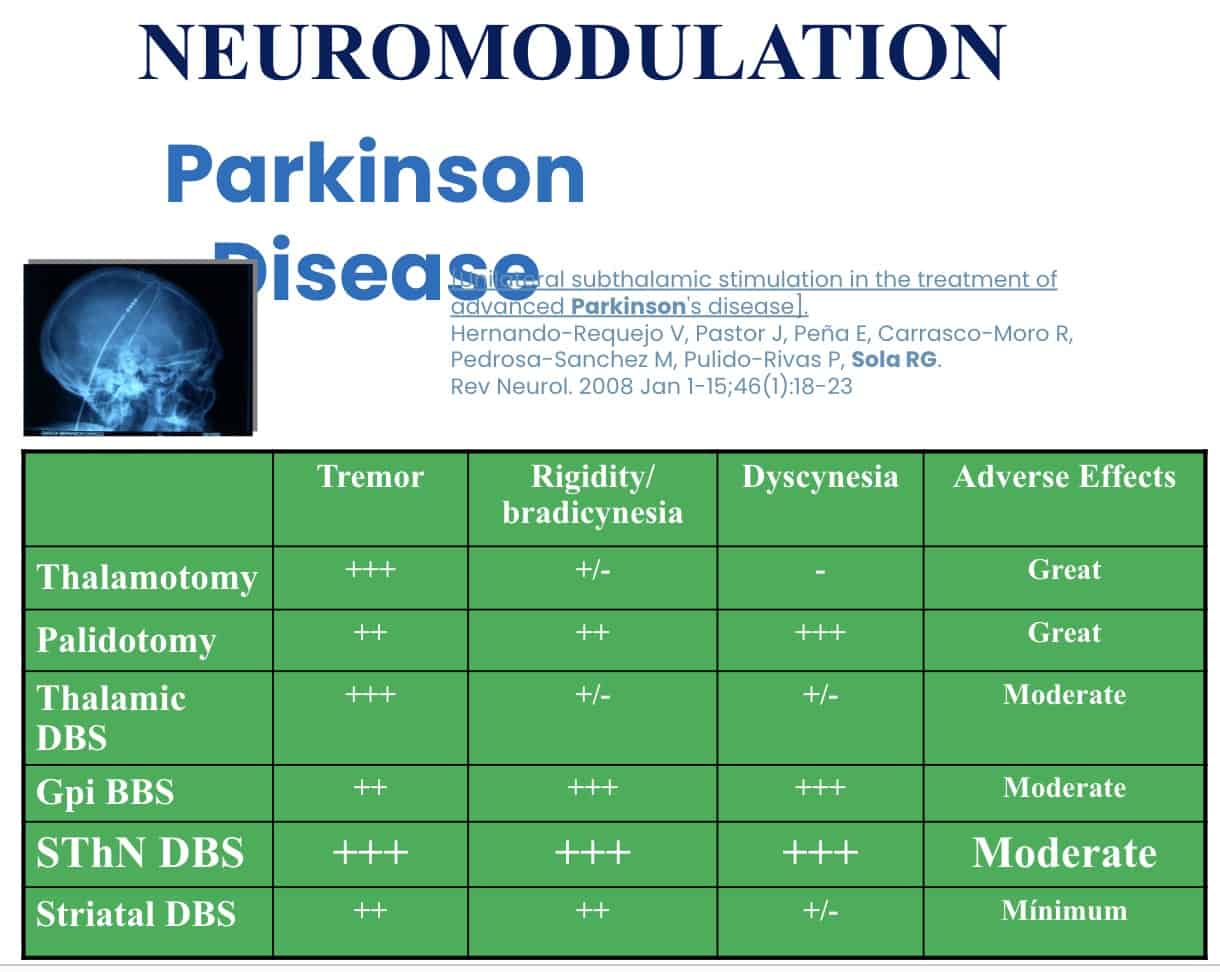
If we review the results of DBS, compared to previous lesion techniques, DBS generates fewer adverse effects.
And among the targets, the subthalamic nucleus is the preferred one.
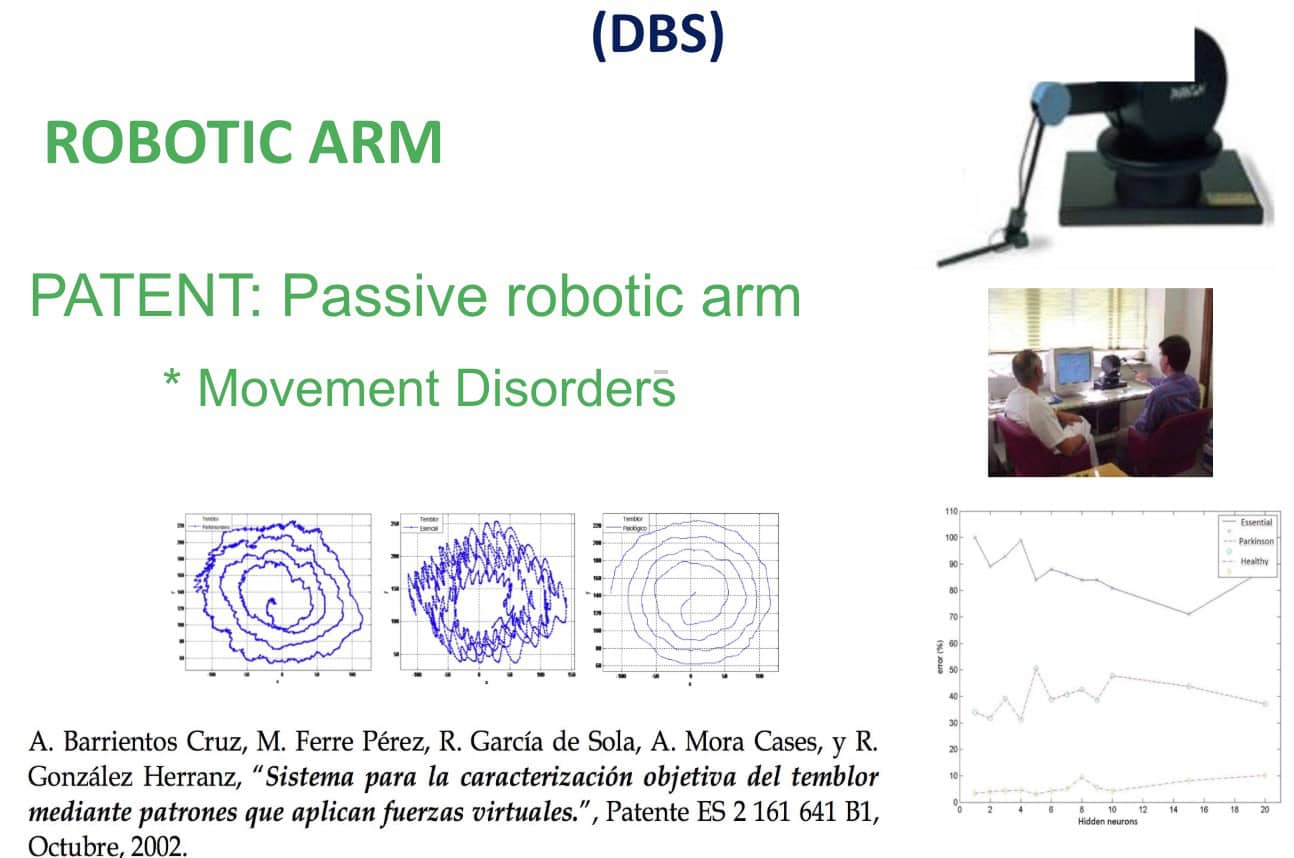
I and an engineering team have developed a new methodology for studying the results of this type of surgical treatment, which was patented in 2002.
We use a passive robotic arm, attached to a finger of the patient’s hand, while the patient performs active movement tests.
This allows us to monitor and record the behavior of the tremor, before and after operating.
B.- Epilepsy Surgery
Another pathology that is treated surgically, when it cannot be controlled with medication, is Epilepsy.
Most surgical interventions are aimed at locating and resecting the epileptogenic zone.
Using, as in this case, the implantation of intracerebral electrodes and recording the epileptogenic activity to clearly demonstrate the onset of epileptic seizures.
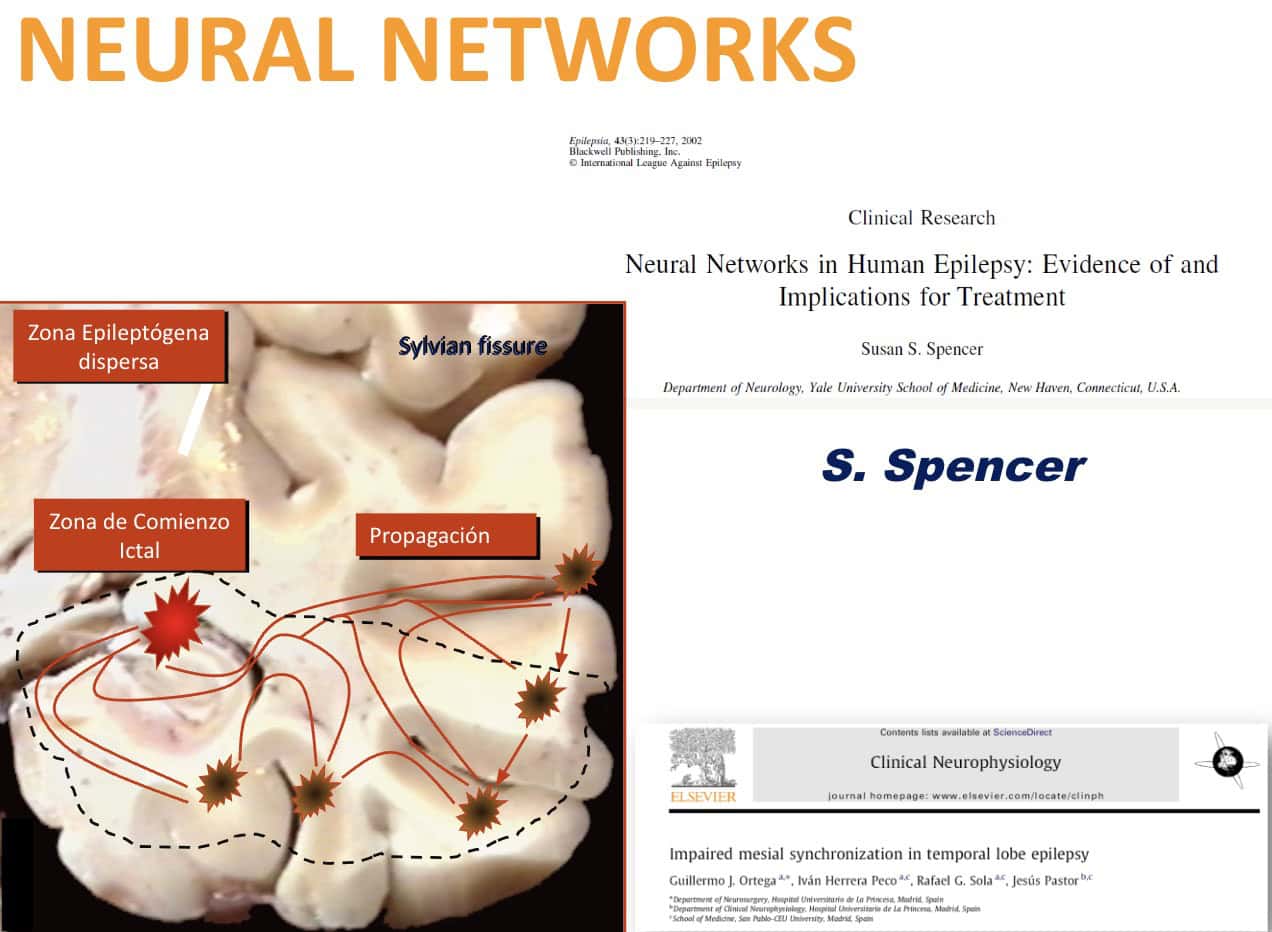
As S. Spencer said, In many cases, when the epileptogenic zone is located in the temporal lobe, the epileptiform activity is like a network.
The experience of many surgeons indicates that, in general, better results are achieved when a large resection including the lateral cortex is performed, as opposed to small and restricted removals of the mesial structures.
With this concept, our group developed different lines of research.
Our data demonstrated the existence of synchronous activity, in the form of a network that emerges from specific areas of the neocortex.
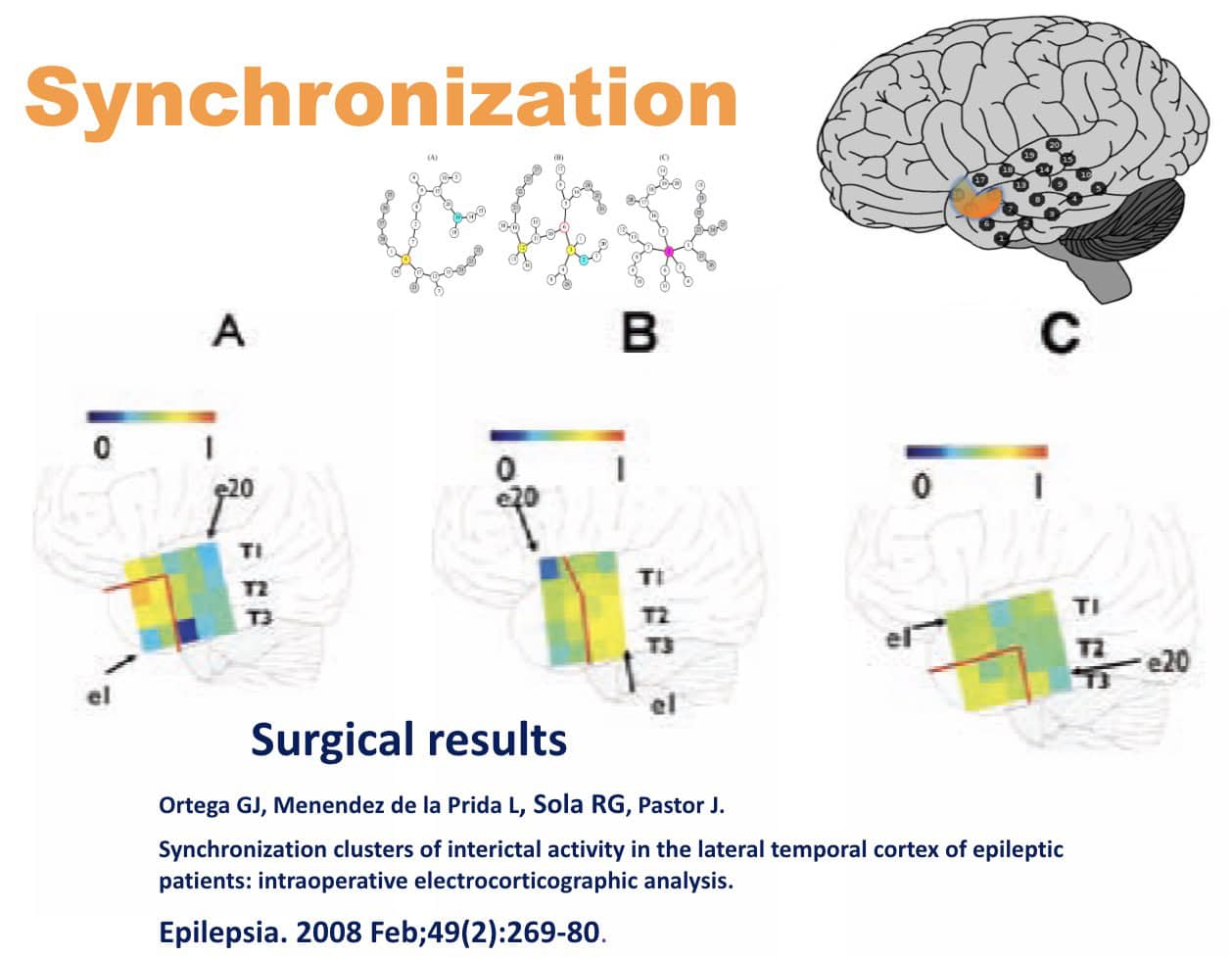
In this image we can see a representation of node synchronization and its relation to post-surgical prognosis in one of our studies.
The red lines indicate the extent of the surgical resection.
The grid shows the cortical interactions.
The blue corresponds to the lack of synchronization, and the red corresponds to perfect synchronization.
In patient A, a well-defined synchronization node was observed within the area that was resected, which included the majority of the synchronized group. Their prognosis was excellent (Engel IA).
Patient B had defined synchronization nodes, which were not excised. Their Engel class was IIB.
Patient C did not clearly show areas of synchronization. Some areas of greater intracortical synchronization were resected, while others remained. Their result was worse, Engel IIIA.
I have just given you a brief overview of cortical resection in focal epilepsy.
Now we will look at neurostimulation.
For half a century now, there have been attempts to control, slow down or abolish the activity of the epileptogenic area by means of electrical stimulation, in very varied areas of the brain.
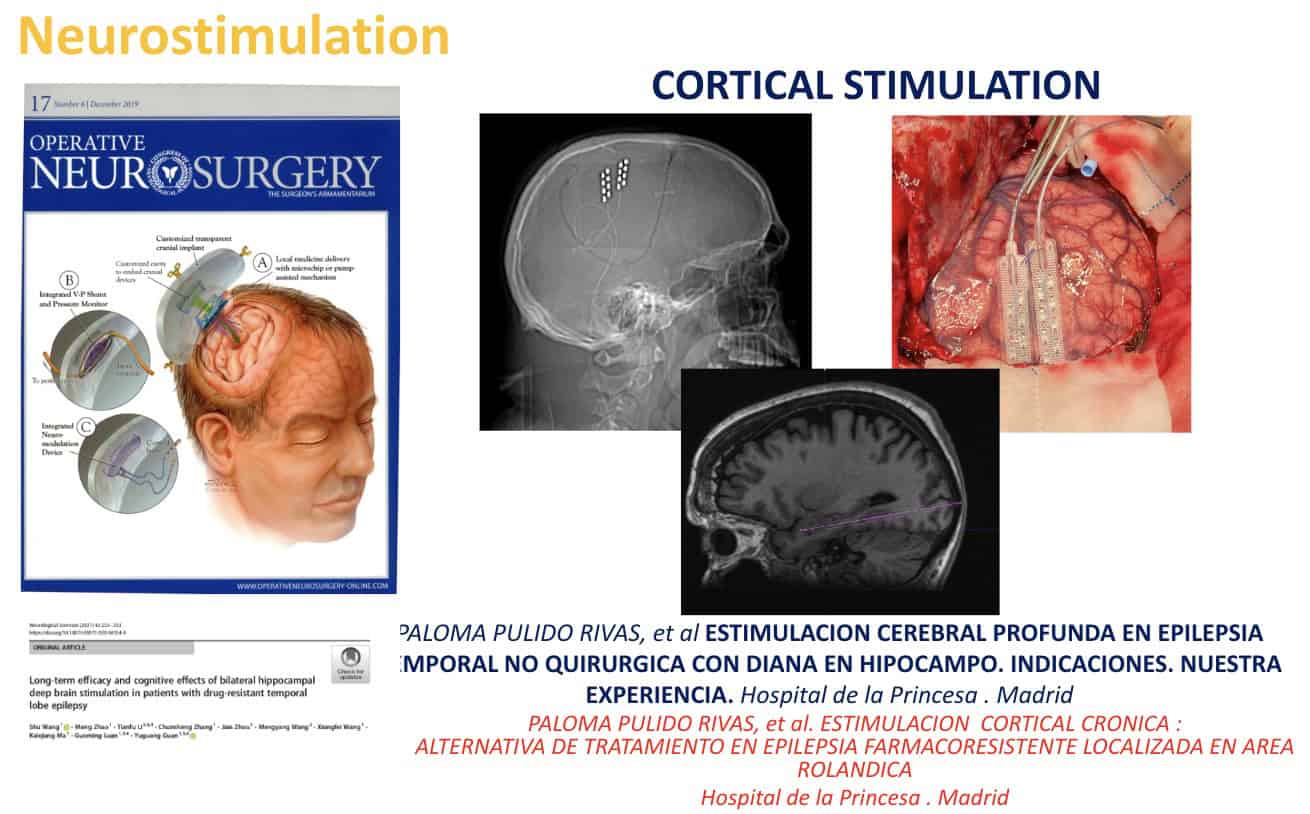
At the present time, there are two forms of neurostimulation.
The first is carried out by means of electrodes implanted in the epileptogenic zone.
This method is currently used in the Epilepsy Surgery Unit of the Hospital de la Princesa.
I started this activity in 1990, until 2017, and it has been continued by Dr. Pulido who is the coordinator of the Unit today.
She recently began performing this new approach.
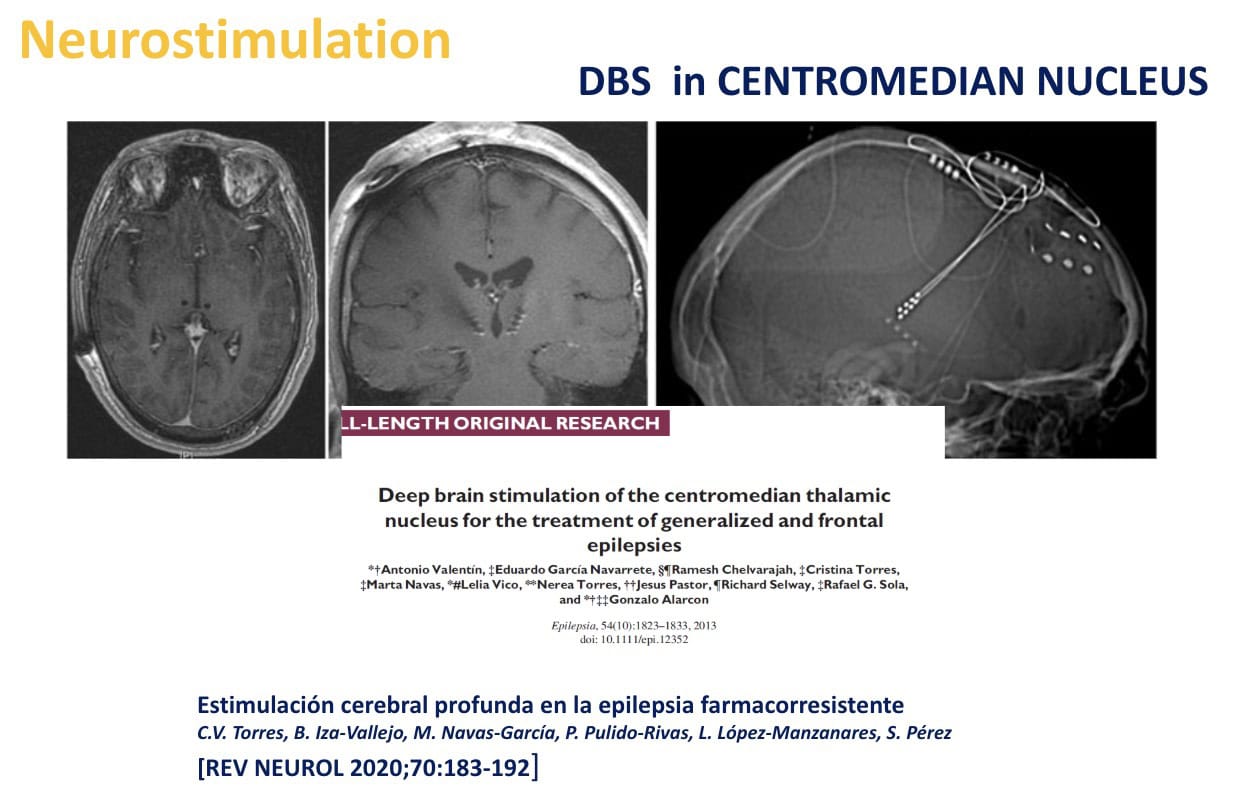
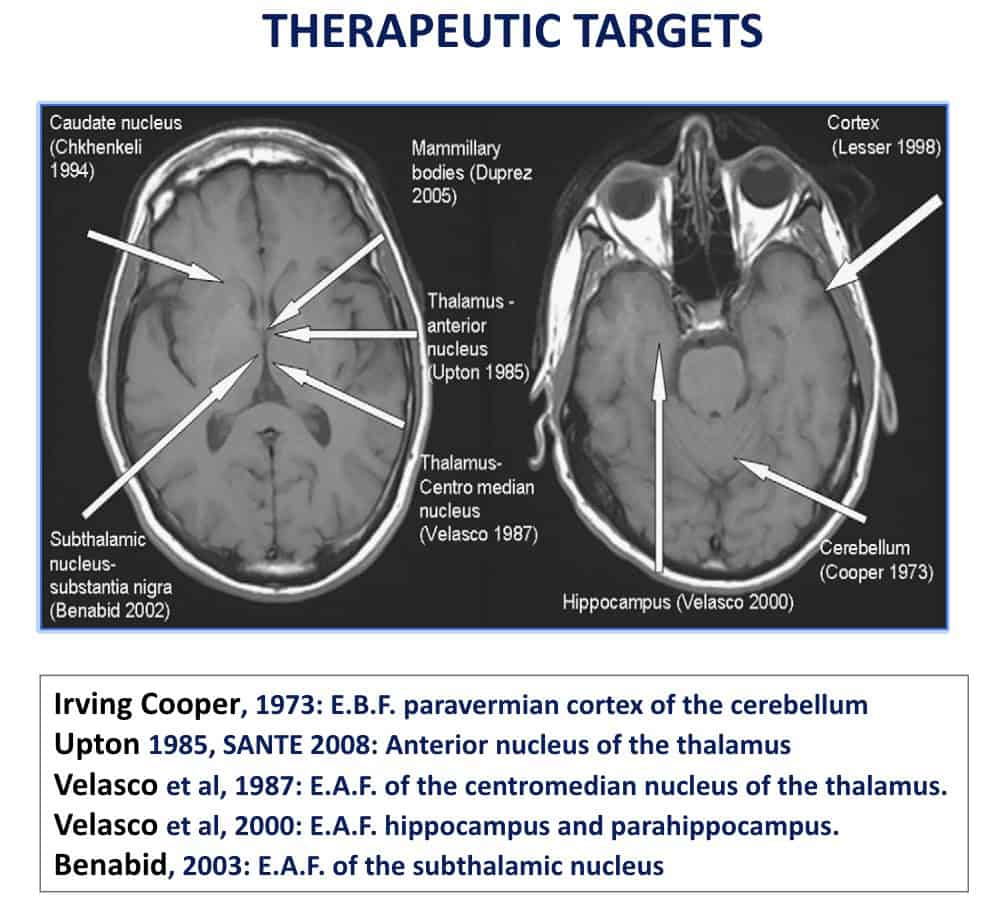
The other way to carry out neurostimulation is in the subcortical structures, normally at the thalamic level, for epilepsies in which there is no easily resectable focus.
As a rule, my team and I choose the Centro-Median Thalamic Nucleus, for multifocal or generalized epilepsies.
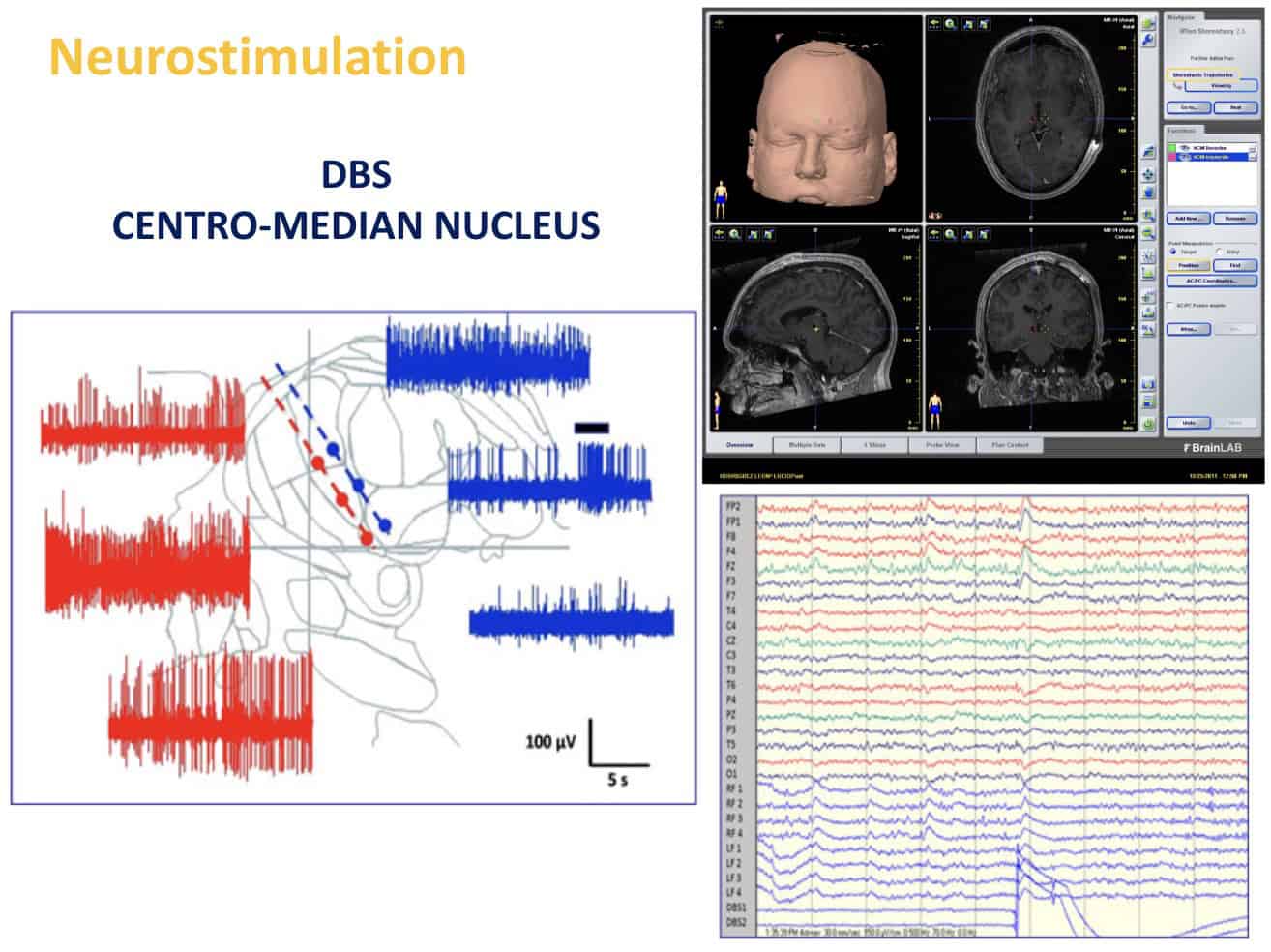
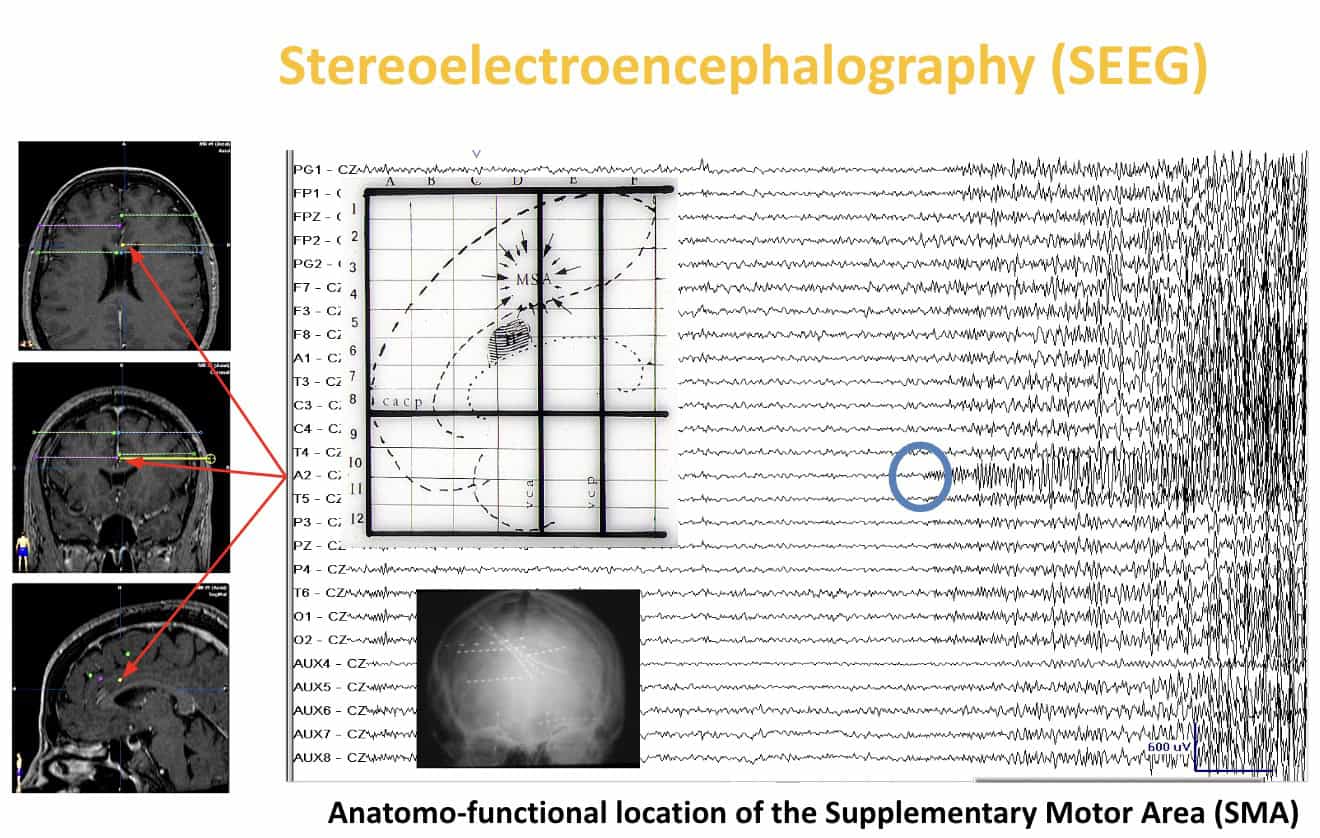
Bilateral DBS electrodes are stereotactically inserted, with electrophysiologic confirmation of their position.
The final electrode position is decided on the basis of atlas-derived coordinates, microelectrode intraoperative recordings, and the thalamic location where stimulation has induced the largest cortical responses.
Let’s look a typical procedure:
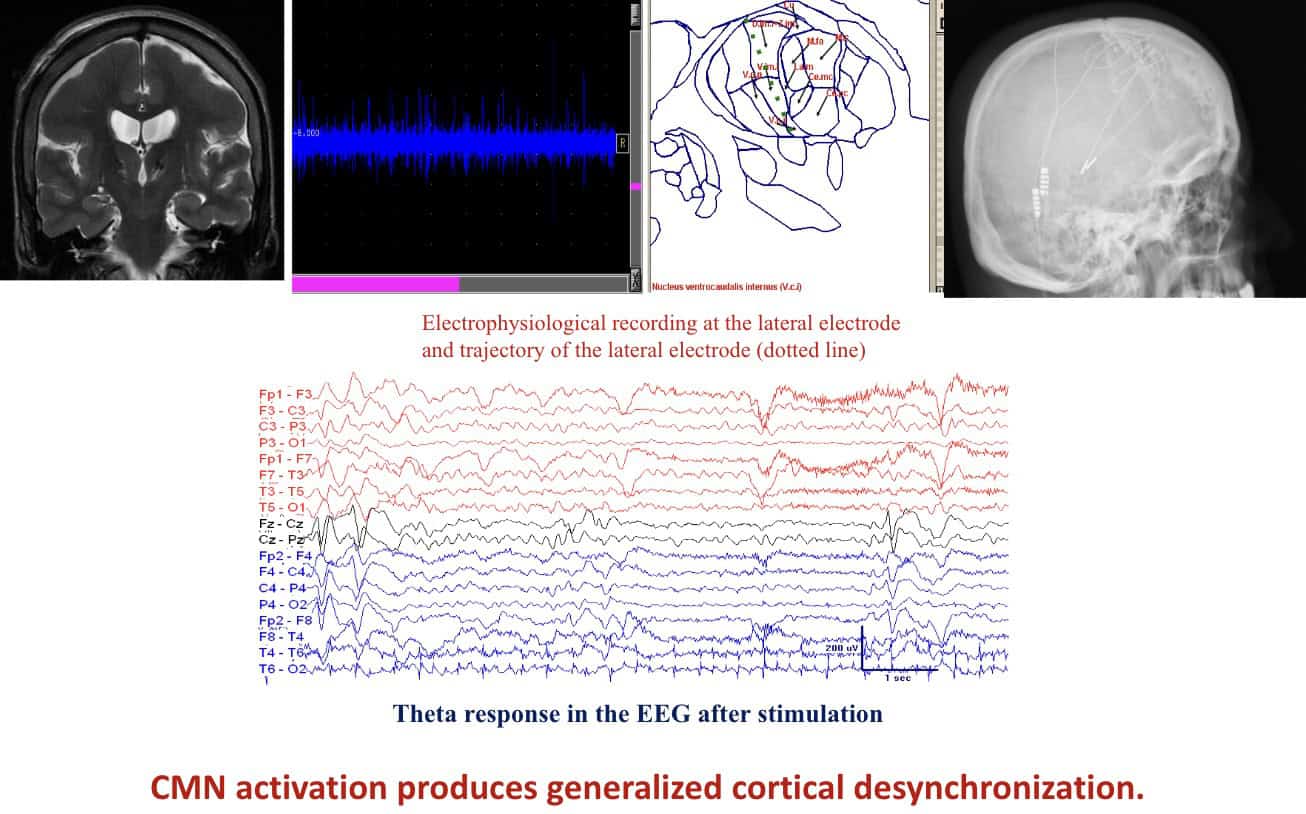
Longitudinal spin echo T1-weighted image shows the position of CMN DBS electrodes in the patient
Neurophysiologic unit gives us recordings as we track to the CMN.
The CMN response is characterized by sparse action potentials of low amplitude.
All patients undergo 1-week scalp video telemetry after DBS electrode implantation in order to identify the optimal DBS stimulation parameters.
The optimal stimulation parameters are identified by the evaluation of seizure frequency and cortical responses to CMN stimulation.
C.- Psychosurgery
A third group of pathologies that are treated surgically are certain severe psychotic disorders.
This type of treatment is called Psychosurgery.
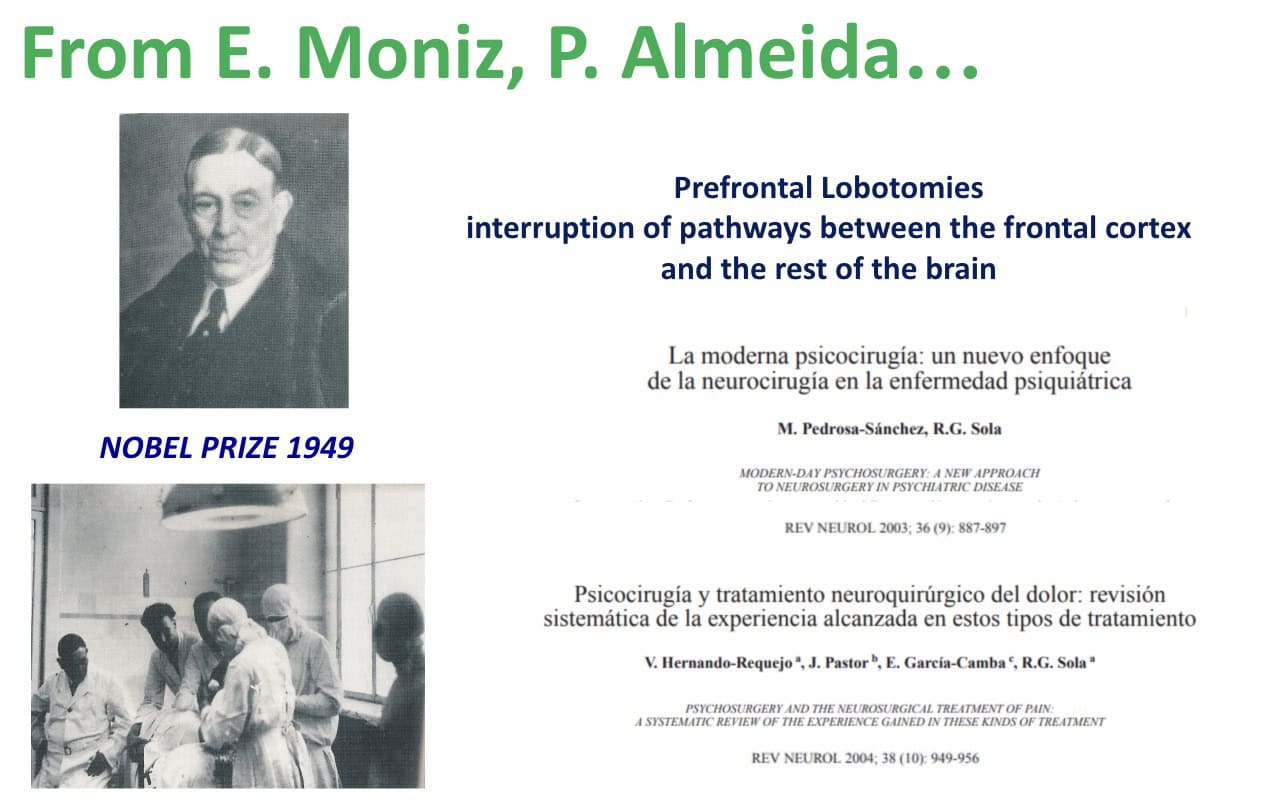
Edgar Moniz gave this type of surgery its name.
He proposed interrupting the communication pathways between the frontal cerebral cortex and the rest of the brain.
In its time, the impact was so great that he received the Nobel Prize.
Spiegel who I mentioned previously, proposed injuring the subcortical nuclei, with a less invasive procedure, to treat patients with very serious psychotic disorders.
For this, he designed and used his stereotactic frame.
The reduction of surgical aggressiveness was significant.
Leksell proposed using non-invasive radiosurgery to carry out these lesions.
In Spain, the work of Dr. Burzaco, with the Gamma Unit in the Ruber International Hospital, must be noted.
Nowadays, in Psychosurgery, as with the treatment of Parkinson’s disease, DBS electrodes are implanted in previously established lesional target to control specific psychotic disorders.
The first application of DBS in Spain in treating a psychiatric condition was carried out by my team in 2006.
The patient was suffering with eretic syndrome (oligophrenia, epilepsy and aggressiveness).
Prior to the operation they had mechanical restraints to the bed for 3 years.
Now, he is able to live under the care of his parents.

We selected the lesional target in the hypothalamus, as proposed by Sano for this type of pathology.
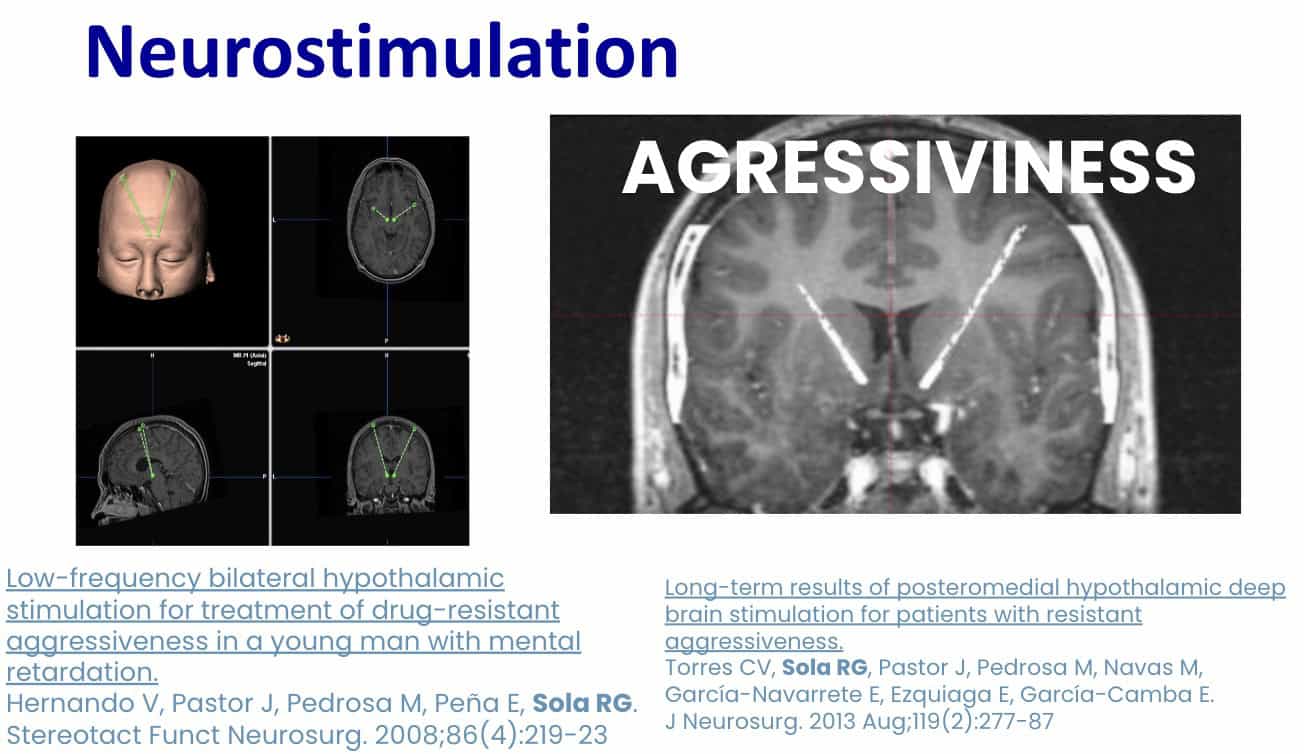
We later published our results regarding other patients that we.treated successfully.

Our group has also gained experience in other psychiatric pathologies, such as depression or obsessive-compulsive disorder.
D.- Pain
The last major group of pathologies treated by DBS is pain.
Like all these types of diseases already mentioned, Neurosurgery began with surgical interventions that removed the structures that caused the painful symptoms.
Often with a component of aggressiveness and high mortality-morbidity.
But there were no adequate medications at that time.
The entire historical journey can be seen in the different medical-surgical treatises on Pain.
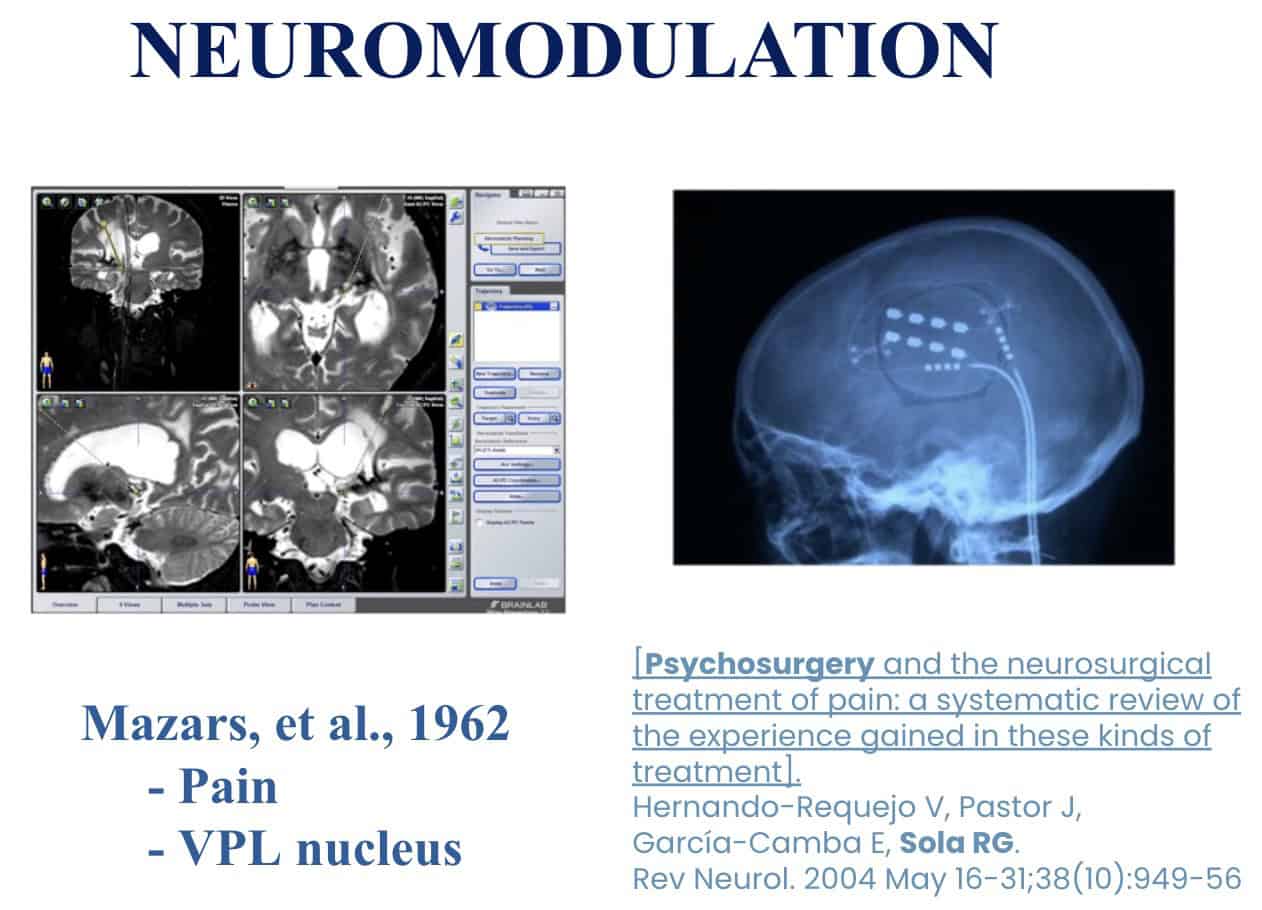
Our group also gained experience in both forms of stimulation treatment.
Either through the Rolandic motor cortex or through stimulation of the thalamic nuclei.
This latter treatment was initiated by Mazard in the 1960s.
We have recently published a review of this whole problem.
Neurostimulation, as in the previous pathologies, can be a very good option in benign chronic pain, especially due to deafferentation or also called central or neuropathic pain.
Thank you for your attention