Analysis of Craniocervical Abnormalities in Osteogenesis Imperfecta during Growth. – Dra. Laura Burgueño-Torres
La Dra Laura Burgueño-Torres, acaba de publicar un artículo en el que analiza la Osteogénesis Imperfecta (OI) como una enfermedad genética caracterizada por osteopenia y fragilidad ósea en la que también se ve afectada la unión craniocervical. Esto es de especial relevancia debido a la alta prevalencia de anomalías descritas en la literatura, tales como invaginación basilar, impresión basilar y platisbasia.
Rafael García de Sola
Director de la Cátedra UAM “Innovación en Neurocirugía”
Jefe del Servicio de Neurocirugía
Hospital Ntra. Sra. del Rosario
Madrid

Published online 2022 Nov 20. doi: MDPI: Analysis of Craniocervical Abnormalities in Osteogenesis Imperfecta during Growth
Manuel Joaquín de Nova-García (Dental Clinical Specialties Department, Faculty of Dentistry, Complutense University of Madrid, 28040 Madrid, Spain).
Rafael García Sola, and Laura Burgueño-Torres
Copyright: © 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/).
Abstract
Osteogenesis Imperfecta (OI) is a genetic disease characterized by osteopenia and bone fragility in which the craniocervical junction is also affected. This is of special relevance due to the high prevalence in anomalies described in the literature as follows: basilar invagination, basilar impression, and platybasia. Methods. We analyzed 19 lateral skull radiographs and 14 magnetic resonance images (MRIs) of 28 patients with OI in which eight linear and five angular measurements were plotted to determine the existence of craniocervical junction anomalies and compare them with 38 lateral skull radiographs and 28 MRIs performed on age-matched healthy controls. Results. From the reference values obtained from the control sample for each age group, we established the limit value at which pathology could be suspected. Some of the variables studied showed a clear trend associated with growth. More than half of the patients (60.71%) presented an anomaly in the skull base. Conclusions. According to the diagnostic criteria used and taking +2.5 SD as the limit value, 10.71% of the patients had basilar invagination, 35.71% had basilar impression, and 39.29% had platybasia, the latter being the most common finding.
Keywords:
osteogenesis imperfecta; craniocervical junction; platybasia; basilar impression; basilar invagination; magnetic resonance imaging
1. Introduction – Craniocervical Abnormalities in Osteogenesis Imperfecta
The craniocervical or craniovertebral junction (CCJ) is a complex transition between the skull and the cervical spine involving two essential neurological structures, which are the brain and the spinal cord; it is formed by the occipital bone and the first two cervical vertebrae [1,2]. Osteogenesis Imperfecta (OI) is a genetic disease characterized by a reduction in bone mass with associated fragility. This bone alteration also affects the CCJ, which is one of the most important complications of OI. It is of special relevance since, in addition to the high prevalence of up to 37% in basilar anomalies in these patients as described in the literature, such deformations of the skull base can compress the brain stem with potentially severe neurological consequences, and they may even become lethal [3]. There are three common anomalies as follows: basilar invagination (protrusion of the odontoid process into the foramen magnum), basilar impression (position of the odontoid process above the caudal borders of the skull without penetrating the foramen magnum), and platybasia, which is defined as the flattening of the skull base [4]. Basilar invagination can be a solitary finding resulting from a number of developmental anomalies, or it can be associated with a more complex developmental process such as Chiari malformation. In the case of basilar impression, the malposition of the odontoid process is secondary to traumatic changes or bone softening in diseases such as OI among others [5]. Platybasia may be associated with basilar impression and basilar invagination. Platybasia alone does not usually cause symptoms unless it is associated with basilar invagination [6].
However, there are few studies in the literature on parallel measurements of struc- tures in voluntary controls [7]. Although data on normal CCJ dimensions and changes in the growth of healthy children are a prerequisite for accurate diagnosis and a better understanding of the development of basilar anomalies, these are scarce. Knowledge of the normal variation in anatomical relationships and the effect of growth at the CCJ is crucial for the diagnosis of pathological conditions in this area. Basilar invagination and basilar impression may originate from skeletal alterations during infancy [3]. In fact, there is evidence that adolescence is the period when there may be progression of basilar impres- sion in children susceptible to CCJ abnormalities, and early intervention may prevent the progressive progression of this anomaly leading to mortality [1].
Basilar impression is considered a frequent complication of OI although the number of cases published up to the 1980s was low [8] possibly because many were asymptomatic. Since the 1980s and 1990s, the neurological complications of OI in the form of basilar impression/invagination and their consequences have been recognized through a higher number of publications. Some of them report symptomatic cases with different neuro- logical manifestations and their complications [9–14]. Others reflect and emphasize their progressiveness to the point that they become another cause of lethality of the disease itself [8,15–18]. Some symptomatic cases presented very early on without any indication of such progressiveness may have also been reported [19]. Many of these cases justify the need for the early detection of such anomalies in order to avoid serious neurological consequences requiring neurosurgical interventions, which do not always limit progression in the affected group [20–22].
The most recent studies reflect a higher number of affected cases. Sawin PD and Menezes AH [23] in 1997 reported the presence of basilar invagination in the 18 patients included in their study based on a classic radiological diagnosis enhanced with computed tomography (CT) and magnetic resonance imaging (MRI). One year later, Engelbert RH et al. [24] confirmed basilar impression in 19% of the children studied (8/42) by radiography and MRI. Janus et al. in 2003 [25] confirmed basilar impression in 6.1% of the cases (8 cases) diagnosed from 130 lateral radiographs with a suspicion of it in 13 cases and confirmation in 8 cases using MRI. The discrepancy between the percentages may reflect not only methodological but also conceptual differences.
The main objective of this study is to analyze the craniocervical junction in patients with OI and compare it with a sample of healthy patients matched by age and sex who present normal cephalometric values for the cranial base. In addition, the aim is to establish the limit values from which pathology is determined in these patients while analyzing the higher or lower frequency of appearance for each of the alterations of the craniocervical junction.
2. Materials and Methods
Study Design
A retrospective cross-sectional study was performed based on a cephalometric analysis of the skull base, lateral skull teleradiography, and brain magnetic resonance imaging (MRI) of children with OI compared with a sample of age- and gender-matched controls without pathologies associated with alterations in the CCJ.
Ethical Aspects
The present study was approved by the Clinical Research Ethics Committee of the San Carlos Clinical Hospital (C.P.-C.I. 13/033-E) as well as by the University Hospital of Getafe (A07-15) in Madrid, Spain, in accordance with the ethical precepts formulated in SAS Order 3470/2009 and the Declaration of Helsinki of the World Medical Association on ethical principles for medical research involving human subjects and its subsequent revisions.
Study Sample and Controls
To be included in the study sample, all participants had to have a diagnosis of OI, a previously performed brain MRI or lateral skull X-ray, an age of up to 18 at the time of the complementary test, and both parental/guardian consent and assent of the minor. Cases in which the MRI or lateral radiographs had not been performed under a standardized protocol or were of insufficient quality to obtain a correct cephalometric diagnosis were excluded. The initial sample consisted of 14 MRIs and 22 lateral skull radiographs (LSRs), with 3 of the latter being excluded in accordance with the exclusion criteria.
For each patient included in the study sample, two age- and gender-matched healthy controls were included in the control sample, providing the imaging tests for the study of the CCJ. The University Hospital of Getafe provided the MRI scans, taking into account the inclusion criteria for the control sample, which included patients without CCJ alterations. A radiological center collaborating with the Faculty of Dentistry of the Complutense University of Madrid provided the LSR, taking into account the same inclusion criteria for the control sample.
All imaging tests were coded according to the Organic Law of Data Protection by a researcher blinded to the research objectives.
Research Systematics
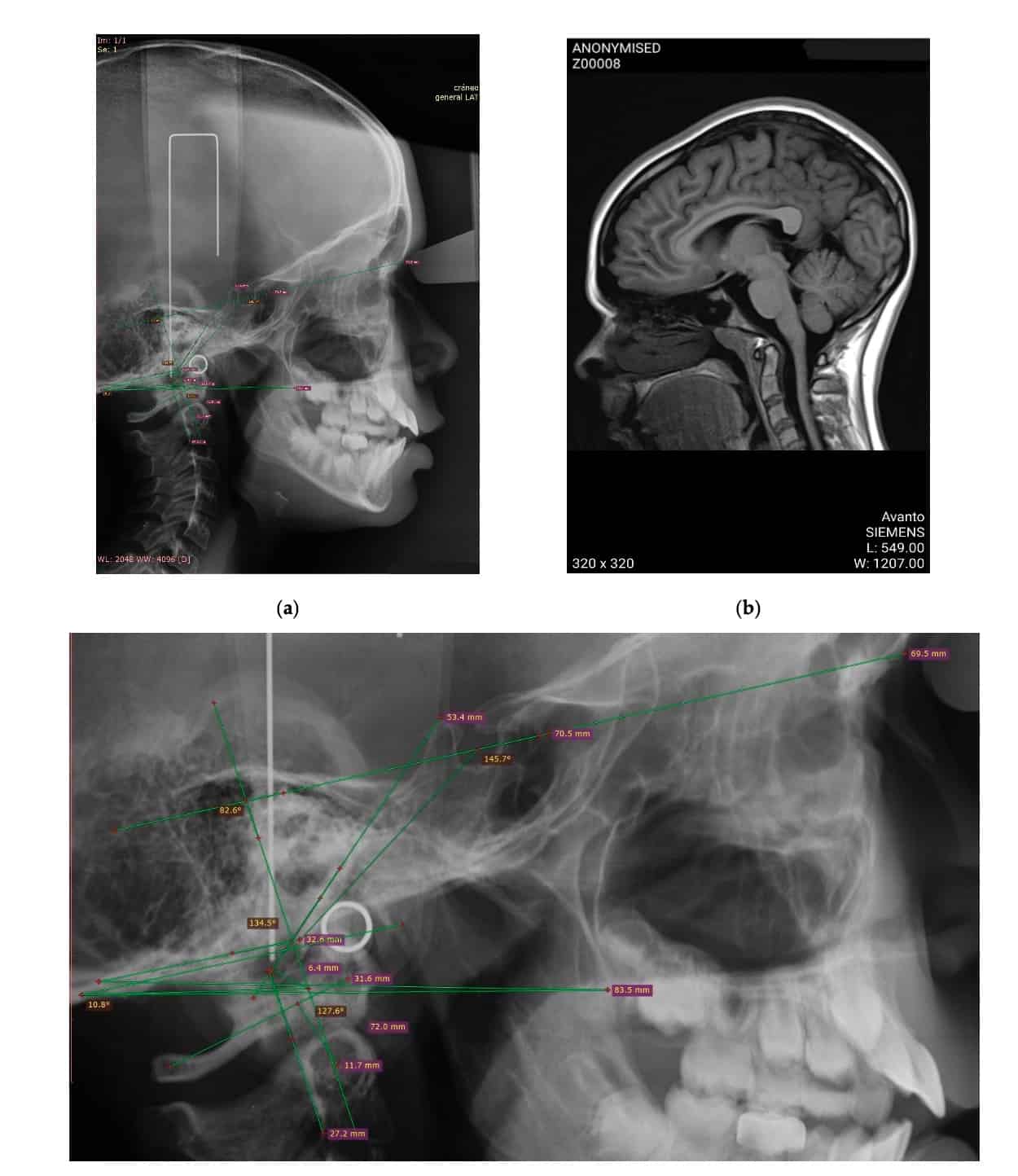
All images were performed following a standardized protocol (Figure 1). The MRIs were reviewed through the PACS program selecting the slices in which the odontoid process was best analyzed. The analysis of the images was carried out by two examiners using RadiAnt DICOM Viewer Software. One of the examiners analyzed the total sample at two different times separated by 15 days, while the second examiner analyzed 30% of the sample, thereby obtaining the inter- and intra-examiner concordance indexes. The total number of images analyzed consisted of 42 MRIs and 57 lateral skull X-rays.
For data collection, 8 linear and 5 angular measurements were analyzed in all the imaging tests included. In the case of the linear measurements, the distance of the odontoid process to the following reference lines was determined, finding positive values when the odontoid process exceeded these lines and the negative values in the opposite case as follows:
- McRae’s line: distance from the anterior and posterior edge of the foramen magnum (Basion and Opisthion).
- Chamberlain’s line: distance from the posterior nasal spine to the Opisthion.
- Modified McGregor: from the posterior nasal spine to the lowest point of the squamosal surface of the occipital.
- Kovero’s line: line parallel to the Nasion–Sella line passing through the most caudal point of the posterior cranial base (point M).
- Wackenheim’s line: perpendicular distance from the posterior border of the odontoid process to the Basion–Sella line.
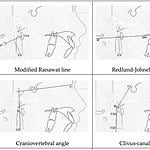
- Ranawat line: perpendicular line running from the center of the axis to the longitudinal axis of the atlas.
- Modified Ranawat line: perpendicular line from the inferior border of the odontoid process to the perpendicular axis of the atlas.
- Redlund–Johnell method: perpendicular distance from the midpoint of the inferior border of the odontoid process to the modified McGregor’s line.
- The angular measurements analyzed were as follows:
- Arponen angle: intersection between the line of Kovero and the line from the tip of the odontoid process to the M point.
- Craniovertebral angle: formed by the Nasion–Sella line and the longitudinal axis of the odontoid process.
- Clivus–canal angle or Wackenheim’s angle: formed by Wackenheim’s line (Sella–Basion) and another line running along the dorsal aspect of the odontoid process.
- Anterior cranial base angle (basal angle): intersection between the Nasion–Sella and Sella–Basion line.
- Boogard’s angle: located between the Sella–Basion–Opisthion points.
Data Analysis
Data analysis was performed with the SPSS program version 22 for Windows, establishing a significance level of p < 0.05. Descriptive statistics were performed for the quantitative and qualitative variables of the sample. The Student’s t-test was also used for the comparison of two means in the case of normal distributions using the Mann–Whitney U test for non-normal distributions. For the comparison of multiple means, ANOVA was employed.
3. Results
Taking into account the inclusion and exclusion criteria, the final study sample consisted of 14 MRIs and 19 LSRs of 28 OI patients aged 6 to 18, which were compared with 38 LSRs and 28 MRIs of age- and gender-matched healthy controls. For higher clarity and the reliability of the results, comparisons were made between groups with the same imaging test (LSR or MRI). The intraclass correlation coefficient was obtained for the intraobserver analysis, obtaining values between 0.81 and 1.00 for almost all the variables except for McRae’s lines (0.79), the Ranawat line (0.79), and Boogard’s angle (0.8) located in the LSR. However, these difficulties were solved by performing the analysis using MRI in which the values obtained in the intraclass correlation coefficient for the intraobserver analysis were 0.95–1.00. The interobserver agreement was almost perfect in all the variables, with indices between 0.81 and 1.00. The second examiner analyzed 30% of the images in the sample; the indices obtained in the interobserver agreement reflect the high reliability of the measurements performed.
Reference Value in the Control Sample
Given that the CCJ changes with growth, Table 1 shows the reference values obtained from the control sample presented by age groups and establishing the limit value of 2.5 SD above which pathology can be suspected.
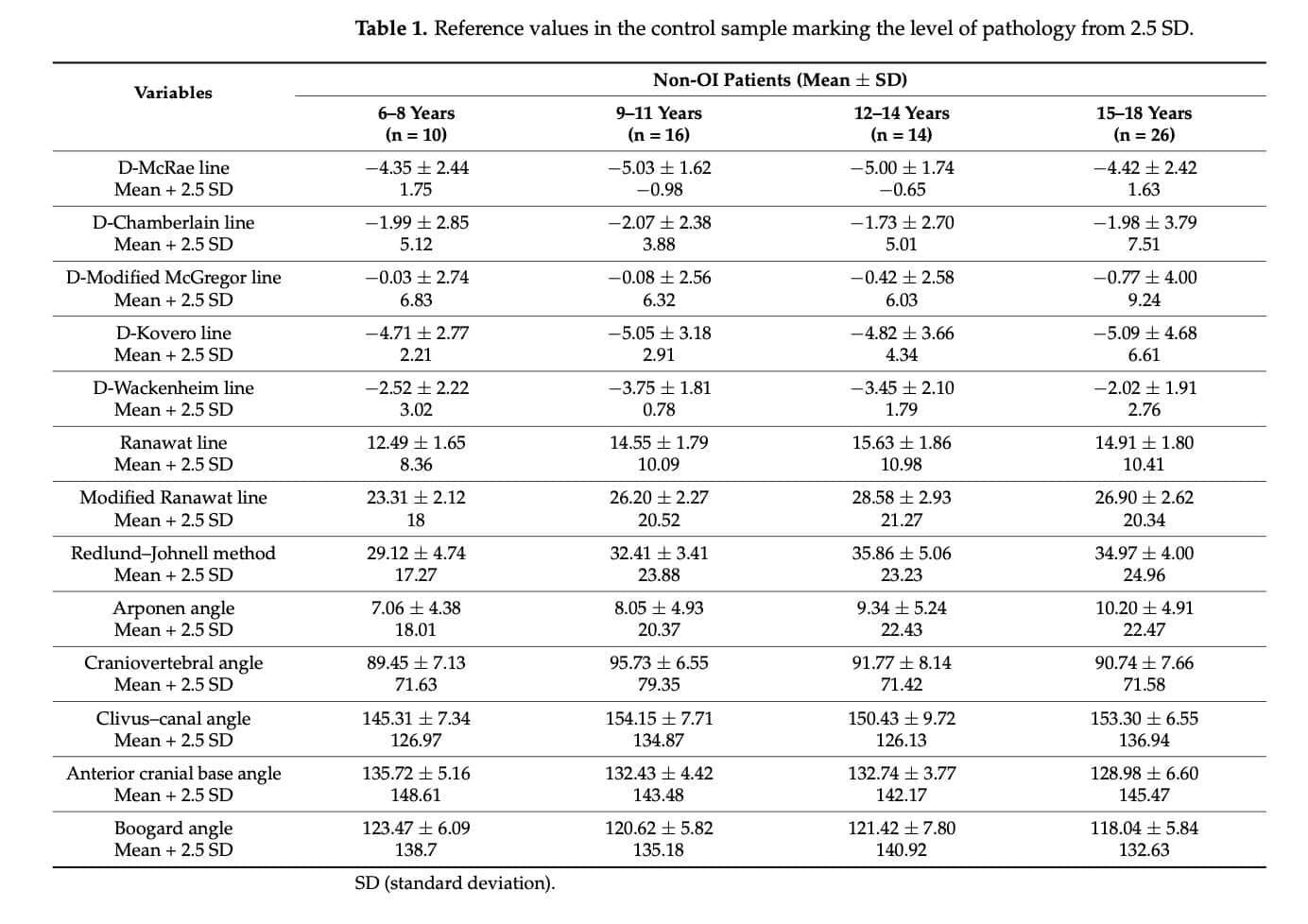
In the light of the data reflected in Table 1, the authors conclude that there are variables such as the McRae D-line, Chamberlain D-line, or Kovero D-line distances that do not show a clear trend associated with growth. However, in the case of the modified D-McGregor’s line, it can be deduced that the odontoid process is more caudal with increasing age with respect to the base of the skull. The Ranawat line as well as the modified Ranawat line increase with growth, stabilizing at 14 years of age and even decreasing thereafter; the same happens with the Redlund–Johnell method.
In the case of measurements such as the Arponen angle, it can be deduced that the odontoid process has a more caudal location with respect to the base of the skull the smaller the patient is, and this becomes closer with growth. The angle of the anterior cranial base decreases with age, with similar values between 9 and 14 years of age.
CCJ Alteration in OI
Taking these values and the pathology limit of 2.5 SD as a reference, 17 of the 28 patients with OI (60.71%) presented some anomalies in the skull base. Three patients had radiographic signs of basilar invagination. All three patients had severe OI, two of them were 9 years old (diagnosis made using MRI) and one was 13 years old (diagnosed on a LSR). The values for these patients were as follows: 0.1 mm and 8.3 mm in the 9-year-old patients and 6.1 mm in the 13-year-old patient.
Several patients in the OI sample met some basilar impression criteria; three patients presented a Chamberlain measurement of >2.5 SD; four were above the McGregor and Kovero measurements; two were above Wackenheim; three presented values that were 2.5 times lower in the Ranawat and 1 in the modified Ranawat; five in the Redlund–Johnell; four were above the Arponen; one was below the craniovertebral angle; and two were below the clivus–canal angle. The means and SD values were obtained from our control sample with matched patients of the same age and gender (Table 2).

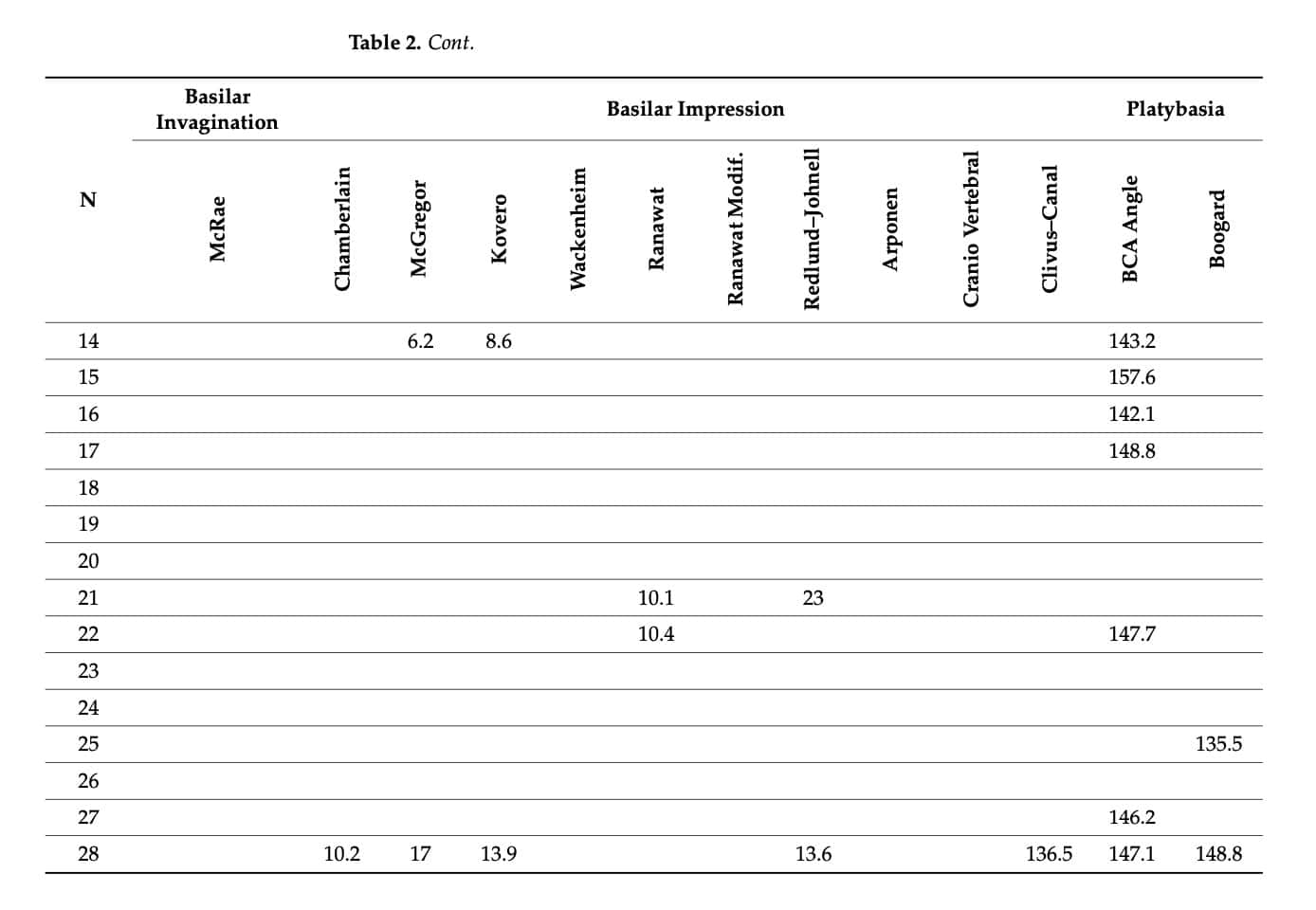
By analyzing how many patients in the OI sample presented platybasia, 9 of the 28 had a basal angle higher than 2.5 SD, and four had a Boogard angle higher than 2.5 standard deviations above the mean of children of the same age (Table 2).
4. Discussion – Analysis of Craniocervical Abnormalities in Osteogenesis Imperfecta
The reliability of CCJ measurements has been analyzed at different moments throughout the literature [3,26,27,28]. Most authors find a greater difficulty in measurements with radiographs given the greater difficulty in the localization of certain anatomical points, such as the Basion and Opisthion points, which has an impact on the measurement of the anterior cranial base angle, McRae’s line, and Chamberlain’s line. For authors such as Arponen et al. [3], these difficulties can be overcome with the measurement of McGregor’s line, which is one of the most reproducible lines of measurement. These authors also conclude that these differences in localization lead to numerical differences in the calculated values although they do not mean major differences. Authors such as Kwong et al. [27] find Wackenheim’s line to be the least reliable of the measurements, and Lee et al. [29] find the greatest difficulties in the McRae and Ranawat lines.
The anatomical points are located in a similar way in LSRs and in MRIs, so the value of the measurements is independent of the image modality [29,30]; however, we found that there are many differences when comparing both diagnostic tests. LSRs have the main disadvantage of overlapping structures, which makes it difficult to determine the location of certain anatomical points, such as the center of the sclerotic ring of the axis. However, these discrepancies are overcome when performing the measurements using MRI since the measurements are more reproducible due to the avoidance of overlapping structures in a 3D image. But, due to the positioning of the patient’s head, there are points that may not be located in the selected slice using MRI since the extension or flexion of the neck modifies the relationship of the odontoid process with other anatomical structures such as the clivus [27], so it is essential that the positioning of the patient’s head follows a protocol both for LSRs and for MRIs. In the present study, we selected the slice in which the most superior point of the odontoid process of the axis, which was the reference for most of the measurements, was best seen. Difficulties were found when locating the most anterior point of the frontonasal suture (Nasion) in the same slice. Therefore, it is important to have all the MRI slices, which serve as the orientation to locate the reference point.
Basilar invagination is studied with the McRae measurement or foramen magnum line. Basilar impression can be analyzed by 10 measurements of which 7 are linear (Chamberlain, modified McGregor, Kovero, Wackenheim, Ranawat, modified Ranawat, Redlund–Johnell) and 3 are angular (Arponen, craniovertebral, clivus–canal). Platybasia can be evaluated by means of the anterior cranial base angle and the Boogard angle [12,23,24,25,30,31,32,33].
The most commonly used reference line is McRae’s line, which determines the anteroposterior dimension of the foramen magnum. In healthy patients, the tip of the odontoid process of the axis should not project above this line [26,33,34,35,36,37,38]. Of the 28 MRIs of the control patients, none have positive values for this line. However, the authors recognize the difficulty in the localization of certain cephalometric points in LSR, as is the case for Basion and Opisthion points, which takes on greater importance at this point in the MRI in which these complications are suppressed. The same happens with Chamberlain’s line, which gives rise to McGregor’s line in which most authors consider a projection above it that is more than 7 mm in the odontoid process to be abnormal [27,39,40,41]. However, authors such as Tassanawipas et al. criticize variables such as Chamberlain’s line and McGregor’s line as they depend on the hard palate, and this can be distorted by an abnormal facial configuration [30]. Kovero’s line eliminates the posterior nasal spine as a reference point in craniovertebral analysis as this anatomical point is modified in patients with orthognathic surgery, which is quite frequent in patients with OI [35]. In the same line of these statements, the authors of the present work agree with other works in the literature and consider that the variations that occur in the base of the skull are also associated with the malocclusion present in patients with OI [42,43] in such a way that in cases of type III and IV OI, the affectation and progression of malocclusion during growth are greater [44].
Angular measurements have also been widely used in the literature for CCJ analysis although some variables, such as the craniovertebral angle, have been less widely used. The present study has obtained a value similar to the one published by Kovero et al. [35], suggesting that this angle remains constant with age.
The anterior cranial base angle is the best indication of platybasia and is frequently associated with basilar invagination and basilar impression [39]. Using the diagnostic criterion of selecting patients with a value of more than 2.5 SD may be clinically important. The value observed for the control sample of the present study was 129.70° ± 6.45° (MRI of the 28 controls, mean 16.32 years) and 133.06° ± 4.87° (LSR of the 38 controls, mean 11.2 years). These results are very similar to those published by Koenigsberg et al. [39], with values of 129° ± 6° for adults and 127° ± 5° for children, and those published by and Kovero et al. [35] with values of 129.8° ± 5.5° for adults. These authors also analyze the Boogard angle, publishing values indicative of platybasia from 126° ± 9.4°.
There are few studies on the anomalies of the CCJ in this disease even though we know that the incidence is high and that the consequences can be fatal. One possible reason for this is that OI is classified as a rare disease, so it can be difficult to find a sufficient sample.
Furthermore, there is no uniformity when cataloguing whether the patient with OI presents pathology or not (Table 3), and the criteria used by the different authors vary from one study to another [4,23,24,25,35,40,42,43,45,46]. The most common diagnosis is considered to be pathological when the odontoid process protrudes more than 5 mm above Chamberlain’s line or more than 7 mm above McGregor’s line, as postulated by Jensen et al. [43]. According to these criteria, 5 of the 28 patients in this study presented values of more than 5 mm at Chamberlain and, of these, 3 also obtained values above 7 mm at McGregor. Authors such as Sawin and Menezes are less strict, considering pathology from 2.5 mm at Chamberlain’s line or 4.5 mm at McGregor’s line [23]. According to this criterion, 9 of the 28 patients in the present study can be considered to present pathological values for Chamberlain’s line and McGregor’s line.
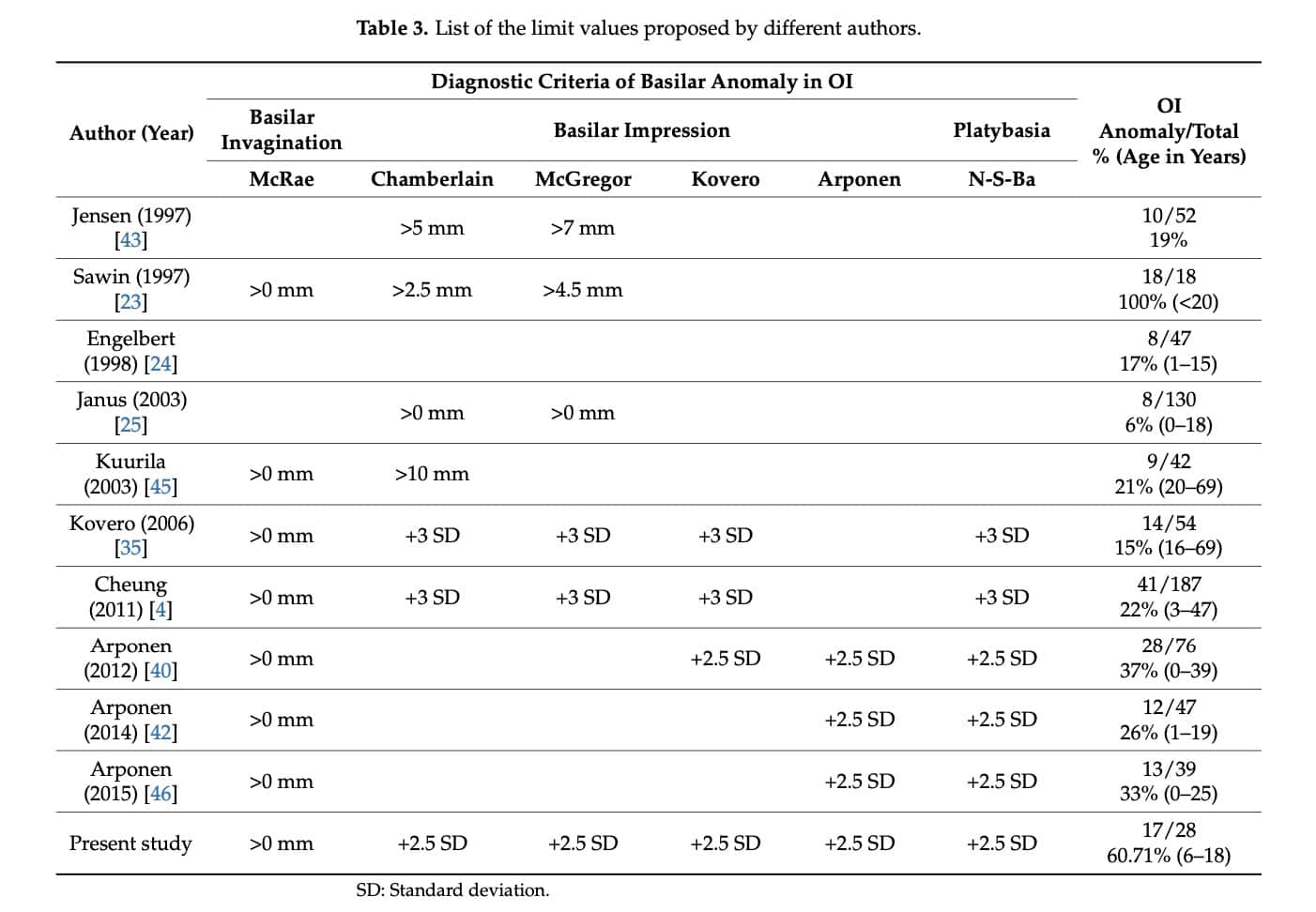
Kovero’s study in 2006 [35] marked a milestone in the diagnosis of CCJ alterations in patients with OI in several ways as follows: It conceptually clarified the three types of alterations studied, which had been recognized as synonyms in previous studies. The researchers also reflected on the importance of applying diagnoses that select the affected patients better, and they left out the control sample. Under these premises, they considered three anomalies of CCJ basilar invagination, basilar impression, and platybasia with a precise definition used for each one, for which they applied more restrictive diagnostic criteria. Thus, in their study sample (54 individuals), they diagnosed 22.2% of the cases of basilar invagination and 11.1% of the cases of platybasia considering +2SD, although +3SD would have more reliably reflected basilar impression, which would have reached 13.2–16.6%. For the diagnosis of basilar impression, they proposed a limit of 3 SD above the mean for the Chamberlain, McGregor, and Kovero measurements (10.6 mm, 11.9 mm, and 9.5 mm, respectively). In the case of platybasia and setting the 3 SD limit, the limit value was 146° for the anterior cranial base angle [35]. According to these criteria, 10 of the 28 patients in the present study present an angle higher than 146°.
In accordance with the presented results, in the sample of children with OI, 9 of the 28 (32.14%) can be considered to have a skull base anomaly if we set the cutoff at +3 SD and by comparing the data with the age-matched controls. Of these 28 children with OI, 5 patients present platybasia, with this being the most common finding, 4 present radiographic signs of basilar impression, and 3 present basilar invagination. In the present study, a lower limit of 2.5 SD is taken as the reference to ensure more sensitive evaluation since in the case of children it is beneficial to identify all the subjects who need a closer follow-up during growth. Following this methodology (+2.5 SD), 17 of the 28 patients with OI (60.71%) can be considered to present an anomaly of the skull base. Of these, 3 patients (10.71%) present basilar invagination, 7 (25%) basilar impression, and 11 (39.29%) platybasia.
Based on Kovero’s study, years later and in a sample of 187 individuals with OI, Cheung MS [4] found that 22% of them presented an abnormality, with platybasia in 16%, basilar impression in 6%, and basilar invagination in 4%. More recently, with the same diagnostic parameters and in the search for an agreement in the monitoring and the follow-up of skull base anomalies in children with OI, Wadanamby S et al. retrospectively studied the data of 94 rx, tomographies, and MRIs; based on the radiographic study, 62% showed platybasia, 11% basilar impression, and 1% basilar invagination [44]. They emphasized the lack of concordance between the diagnostic methods (radiographs and MRIs). Although there is higher diagnostic accuracy whenb using MRI, they reserved it for confirming the diagnosis of symptomatic cases or when radiographic parameters were abnormal.
5. Conclusions
The variables analyzed in this study of the CCJ are directly related to the identification of the different anatomical points, so reliability depends on accurate location.
In existing studies in the literature, the diagnostic criteria used to determine the presence or absence of pathology in the CCJ are different. In the work presented here, we have taken +2.5 SD as the limit value for the variables analyzed. According to this, 60.71% of the OI patients presented an anomaly of the skull base, 10.71% basilar invagination, 35.71% basilar impression, and 39.29% platybasia, with the latter being the most common finding.
6. Study Limitations
The intrinsic limitations of measuring lateral skull radiographs should be emphasized, and the authors opted for measurements by two examiners for this reason, thereby achieving inter- and intra-examiner concordance. However, the fact that these images were available for orthodontic and malocclusion diagnosis provided the advantage of being able to use them for the analysis of the CCJ.
Furthermore, although all the diagnostic tests were performed under a standardized protocol, they were not performed at the same center since the authors did not request the performance of any of these radiographic examinations for the purpose of their inclusion in the study.
Furthermore, we have to take into account that OI is a rare disease with a low prevalence. Furthermore, the patients included in the study come to the Faculty of Dentistry for reasons other than the study of CCJ alterations, so obtaining a large sample is a major difficulty.
Author Contributions
Conceptualization, M.J.D.N.-G.; methodology, M.J.D.N.-G. and R.G.S.; software, R.G.S.; validation, L.B.-T.; formal analysis, L.B.-T.; investigation, M.J.D.N.-G. and L.B.-T.; resources, R.G.S.; data curation, L.B.-T.; writing—original draft preparation, L.B.-T.; writing—review and editing, M.J.D.N.-G.; visualization, L.B.-T.; supervision, R.G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the San Carlos Clinic Hospital (C.P.-C.I. 13/033-E, approved on 22 February 2013) and the Ethics Committee of the University Hospital of Getafe (A07-15, approved on 3 June 2015).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author upon reasonable request.
Acknowledgments
This study was made possible by support from the AHUCE Foundation, which helps to improve both quality of life and care for these patients by sponsoring research in the field of Osteogenesis Imperfecta. The authors are grateful for the collaboration of the Radiology Service of the University Hospital of Getafe (Madrid), which provided the MRI scans of the control sample matched with the OI patients. The authors are also grateful for the collaboration of the Oral and Facial Diagnostic Center, which provided the lateral skull radiographs of the control sample.
Conflicts of Interest
The authors declare no conflicts of interest.
References
1. Menezes, A.H.; Traynelis, V.C. Anatomy and biomechanics of normal craneovertebral junction (a) and biomechanics of stabilization (b). Childs Nerv. Syst. 2008, 24, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
2. Benke, M.; Yu, W.D.; Peden, S.C.; O’Brien, J.R. Occipitocervical Junction: Imaging, Pathology, Instrumentation. Am. J. Orthop. 2011, 40, E205–E215. [Google Scholar] [PubMed]
3. Arponen, H.; Elf, H.; Evälahti, M.; Waltimo-Sirén, J. Reliability of cranial base measurements on lateral skull radiographs. Orthod. Craniofacial Res. 2008, 11, 201–210. [Google Scholar] [CrossRef] [PubMed]
4. Cheung, M.S.; Arponen, H.; Roughley, P.; Azouz, M.E.; Glorieux, F.H.; Waltimo-Sirén, J.; Rauch, F. Cranial base abnormalities in osteogenesis imperfecta: Phenotypic and genotypic determinants. J. Bone Miner. Res. 2011, 26, 405–413. [Google Scholar] [CrossRef]
5. Pinter, N.K.; McVige, J.; Mechtler, L. Basilar Invagination, Basilar Impression, and Platybasia: Clinical and Imaging Aspects. Curr. Pain Headache Rep. 2016, 20, 49. [Google Scholar] [CrossRef] [PubMed]
6. Chen, Y.; Liu, H. Imaging of Craniovertebral Junction. Neuroimage Clin. N. Am. 2009, 19, 483–510. [Google Scholar] [CrossRef]
7. Arponen, H.; Evälahti, M.; Waltimo-Sirén, J. Dimensions of the craniocervical junction in longitudinal analysis of normal growth. Child’s Nerv. Syst. 2010, 26, 763–769. [Google Scholar] [CrossRef]
8. Pozo, J.; Crockard, H.; Ransford, A. Basilar impression in osteogenesis imperfecta. A report of three cases in one family. J. Bone Jt. Surg. 1984, 66-B, 233–238. [Google Scholar] [CrossRef]
9. Frank, E.; Berger, T.; Tew, J.M. Basilar impression and platybasia in osteogenesis imperfecta tarda. Surg. Neurol. 1982, 17, 116–119. [Google Scholar] [CrossRef]
10. Sillence, D.O. Craniocervical abnormalities in osteogenesis imperfecta: Genetic and molecular correlation. Pediatr. Radiol. 1994, 24, 427–430. [Google Scholar] [CrossRef] [PubMed]
11. Reilly, M.M.; Valentine, A.R.; Ginsberg, L. Trigeminal neuralgia associated with osteogenesis imperfecta. J. Neurol. Neurosurg. Psychiatry 1995, 58, 665. [Google Scholar] [CrossRef]
12. Hayes, M.; Parker, G.; Ell, J.; Sillence, D. Basilar impression complicating osteogenesis imperfecta type IV: The clinical and neuroradiological findings in four cases. J. Neurol. Neurosurg. Psychiatry 1999, 66, 357–364. [Google Scholar] [CrossRef]
13. Al Kaissi, A.; Klaushofer, K.; Grill, F. Distinctive tomographic abnormalities of the craniocervical region in a patient with osteogensis imperfecta type IV B. Clinics 2010, 65, 647–649. [Google Scholar] [CrossRef] [PubMed]
14. Ghosh, P.S.; Taute, C.T.; Ghosh, D. Teaching neuro images: Platybasia and basilar invagination in osteogenesis imperfecta. Neurology 2011, 77, e108. [Google Scholar] [CrossRef] [PubMed]
15. Pauli, R.M.; Gilbert, E.F. Upper cervical cord compression as cause of death in osteogenesis imperfecta type II. J. Pediatr. 1986, 108, 574–581. [Google Scholar] [CrossRef] [PubMed]
16. Kurimoto, M.; Ohara, S.; Takaku, A. Basilar impression in osteogenesis imperfecta tarda: Case report. J. Neurosurg. 1991, 74, 136–138. [Google Scholar] [CrossRef] [PubMed]
17. McAllion, S.J.; Paterson, C.R. Causes of death in osteogenesis imperfecta. J. Clin. Pathol. 1996, 49, 627–630. [Google Scholar] [CrossRef]
18.- De Nova-García, M.J.; Sola, R.G.; Burgueño-Torres, L. Influence of the Severity of Osteogenesis Imperfecta on Cranial Measurements. Children 2023, 10, 1029. [Google Scholar] [CrossRef]
19. Rush, P.J.; Berbrayer, D.; Reilly, B.J. Basilar impression and osteogenesis imperfecta in a three-year-old girl: CT and MRI. Pediatr. Radiol. 1989, 19, 142–143. [Google Scholar] [CrossRef]
20. Ibrahim, A.G.; Crockard, H.A. Basilar impression and osteogenesis imperfecta: A 21-year retrospective review of outcomes in 20 patients. J. Neurosurg. Spine 2007, 7, 594–600. [Google Scholar] [CrossRef]
21. Menezes, A.H. Specific entities affecting the craniocervical region. Osteogenesis imperfecta and related osteochondrodysplasias: Medical and surgical management of basilar impression. Child’s Nerv. Syst. 2008, 24, 1169–1172. [Google Scholar] [CrossRef]
22. Sasaki-Adams, D.; Kulkarni, A.; Rutka, J.; Dirks, P.; Taylor, M.; Drake, J.M. Neurosurgical implications of osteogenesis imperfecta in children. Report of 4 cases. J. Neurosurg. Pediatr. 2008, 1, 229–236. [Google Scholar] [CrossRef] [PubMed]
23. Sawin, P.D.; Menezes, A.H. Basilar invagination in osteogenesis imperfecta and related osteochondrodysplasias: Medical and surgical management. J. Neurosurg. 1997, 86, 950–960. [Google Scholar] [CrossRef]
24. Engelbert, R.H.H.; Gerver, W.J.M.; Breslau-Siderius, L.J.; van der Graaf, Y.; Pruijs, H.E.H.; van Doorne, J.M.; Beemer, F.A.; Helders, P.J.M. Spinal complications in osteogenesis imperfecta 47 patients 1–16 years of age. Acta Orthop. Scand. 1998, 69, 283–286. [Google Scholar] [CrossRef] [PubMed]
25. Janus, G.; Engelbert, R.; Beek, E.; Gooskens, R.; Pruijs, J. Osteogenesis imperfecta in childhood: MR imaging of basilar impression. Eur. J. Radiol. 2003, 47, 19–24. [Google Scholar] [CrossRef]
26. Soni, P.; Sharma, V.; Sengupta, J. Cervical vertebrae anomalies—Incidental findings on lateral cephalograms. Angle Orthod. 2008, 78, 176–180. [Google Scholar] [CrossRef]
27. Kwong, Y.; Rao, N.; Latief, K. Craniometric measurements in the assessment of craniovertebral settling: Are they still relevant in the age of cross-sectional imaging? Am. J. Roentgenol. 2011, 196, W421–W425. [Google Scholar] [CrossRef] [PubMed]
28. McRae, D.L. Bony abnormalities in the region of the foramen magnum: Correlation of the anatomic and neurologic findings. Acta Radiol. 1953, 40, 335–354. [Google Scholar] [CrossRef] [PubMed]
29. Lee, H.J.; Hong, J.T.; Kim, I.S.; Kwon, J.Y.; Lee, S.W. Analysis of measurement accuracy for craniovertebral junction pathology: Most reliable method for cephalometric analysis. J. Korean Neurosurg. Soc. 2013, 54, 275–279. [Google Scholar] [CrossRef] [PubMed]
30. Tassanawipas, A.; Mokkhavesa, S.; Chatchavong, S.; Worawittayawong, P. Magnetic resonance imaging study of the craniocervical junction. J. Orthop. Surg. 2005, 13, 228–231. [Google Scholar] [CrossRef]
31. Cronin, C.; Lohan, D.; Ni Mhuircheartigh, J.; Meehan, C.; Murphy, J.; Roche, C. MRI evaluation and measurement of the normal odontoid peg position. Clin. Radiol. 2007, 62, 897–903. [Google Scholar] [CrossRef] [PubMed]
32. Cronin, C.; Lohan, D.; Mhuircheartigh, J.; Meehan, C.; Murphy, J.; Roche, C. CT evaluation of Chamberlain’s, McGregor’s, and McRae’s skull-base lines. Clin. Radiol. 2009, 64, 64–69. [Google Scholar] [CrossRef] [PubMed]
33. Smoker, W.R.K.; Khanna, G. Imaging the craniocervical junction. Child’s Nerv. Syst. 2008, 24, 1123–1145. [Google Scholar] [CrossRef] [PubMed]
34. Hansen, M.A.; da Cruz, M.J.; Owler, B.K. Endoscopic transnasal decompression for management of basilar invagination in osteogenesis imperfecta. J. Neurosurg. Spine 2008, 9, 354–357. [Google Scholar] [CrossRef] [PubMed]
35. Kovero, O.; Pynnönen, S.; Kuurila-Svahn, K.; Kaitila, I.; Waltimo-Sirén, J. Skull base abnormalities in osteogenesis imperfecta: A cephalometric evaluation of 54 patients and 108 control volunteers. J. Neurosurg. 2006, 105, 361–370. [Google Scholar] [CrossRef] [PubMed]
36. Aldana, A.; Báez, J.; Sandoval, C.; Vergara, C.; Cauvi, D.; Fernández de la Reguera, A. Asociación entre maloclusiones y posición de cabeza y cuello [Association between malocclusion and position of the head and neck]. Int. J. Odontostomat. 2011, 5, 119–125. [Google Scholar] [CrossRef]
37. Heredia Rizo, A.M.; Albornoz Cabello, M.; Piña Pozo, F.; Luque Carrasco, A. La postura del segmento craneocervical y su relación con la oclusión dental y la aplicación de ortodoncia: Estudio de revisión. [Craniocervical segment posture and its relationship to dental occlusion and orthodontic application: A review study]. Osteopat. Científica 2010, 5, 89–96. [Google Scholar] [CrossRef]
38. De Nova-García, M.J.; Bernal-Barroso, F.; Mourelle-Martínez, M.R.; Gallardo-López, N.E.; Diéguez-Pérez, M.; Feijoo-García, G.; Burgueño-Torres, L. Evaluation of the Severity of Malocclusion in Children with Osteogenesis Imperfecta. J. Clin. Med. 2022, 11, 4862. [Google Scholar] [CrossRef]
39. Koenigsberg, R.A.; Vakil, N.; Hong, T.A.; Htaik, T.; Faerber, E.; Maiorano, T.; Dua, M.; Faro, S.; Gonzales, C. Evaluation of Platybasia with MR Imaging. AJNR Am. J. Neuroradiol. 2005, 26, 89–92. [Google Scholar]
40. Arponen, H.; Mäkitie, O.; Haukka, J.; Ranta, H.; Ekholm, M.; Mäyränpää, M.K.; Kaitila, I.; Waltimo-Sirén, J. Prevalence and natural course of craniocervical junction anomalies during growth in patients with osteogenesis imperfecta. J. Bone Miner. Res. 2012, 27, 1142–1149. [Google Scholar] [CrossRef]
41. Vieira, R.; Zandonadi, E.D. Angular craniometry in craniocervical junction malformation. Neurosurg. Rev. 2003, 36, 603–610. [Google Scholar]
42. Arponen, H.; Mäkitie, O.; Waltimo-Sirén, J. Association between joint hypermobility, scoliosis, and cranial base anomalies in paediatric Osteogenesis imperfecta patients: A retrospective cross-sectional study. MC Musculoskelet. Disord. 2014, 15, 428. [Google Scholar] [CrossRef] [PubMed]
43. Jensen, B.L.; Lund, A. Osteogenesis imperfecta: Clinical, cephalometric, and biochemical investigations of OI types I, III, and IV. J. Craniofac. Genet. Dev. Biol. 1997, 17, 121–132. [Google Scholar]
44. Wadanamby, S.; El Garwany, S.; Connolly, D.; Arundel, P.; Bishop, N.; DeVile, C.; Calder, A.; Crowe, B.; Burren, C.; Saraff, V.; et al. Monitoring skull base abnormalities in children with osteogenesis imperfecta—Review of current practice and a suggested clinical pathway. Bone 2022, 154, 116235. [Google Scholar] [CrossRef] [PubMed]
45. Kuurila, K.; Kentala, E.; Karjalainen, S.; Pynnönen, S.; Kovero, O.; Kaitila, I.; Grénman, R.; Waltimo, J. Vestibular dysfunction in adult patients with osteogenesis imperfecta. Am. J. Med. Genet. Part A 2003, 120A, 350–358. [Google Scholar] [CrossRef]
46. Arponen, H.; Vuorimies, I.; Haukka, J.; Valta, H.; Waltimo-Sirén, J.; Mäkitie, O. Cranial base pathology in pediatric osteogenesis imperfecta patients treated with bisphosphonates. J. Neurosurg. Pediatr. 2015, 15, 313–320. [Google Scholar] [CrossRef]