Deep brain stimulation of the subcallosal cingulate for medication-resistant type I bipolar depression
Hospital Universitario La Princesa – Madrid
case report
Patients with unipolar depression have been reported as having derived benefit from deep brain stimulation (DBS) of the subcallosal cingulate (1 – 8). Experience with DBS for bipolar depression is scarce, and limited to patients with type II bipolar depression (1 – 8). We present the first case of type I bipolar disorder successfully treated with DBS of this area.
The patient was a 78-year-old woman diagnosed with DSM-IV recurrent and severe type I bipolar depression, without other comorbid disorders. She was initially diagnosed with unipolar depression in 1984, but she gradually developed clinically significant episodes of mania for which lithium was introduced in 1995 with an initial irregular compliance. Since that time, she had experienced multiple relapses of depression and manic episodes, requiring frequent admissions to the acute psychiatric unit. Response to treatment with various stabilizers (constant lithium, valproate, and lamotrigine), antipsychotics (olanzapine, quetiapine, pimozide, and haloperidol), and antidepressants (dual, selective serotonin reuptake inhibitors), alone and in combinations, was poor. In 2009, she developed a severe depressive episode that persisted for two years, with mood-congruent psychotic symptoms (Cotard syndrome), despite good adherence to treatment for several years previously. Other drugs such as quetiapine, pimozide, escitalopram, or bupropion were also administered at effective doses. Several admissions to the hospital for electroconvulsive therapy (a total of 42 sessions) were required, with limited clinical response. Therefore, she was considered for DBS.
Our local ethics committee approved the surgical treatment and informed consent was obtained from the patient and her family. The patient underwent brain magnetic resonance imaging (MRI) and a complete neuropsychological evaluation, which did not show any significant abnormalities (her scores at Mini-Mental State Examination were 29/30). Preoperatively, she was taking quetiapine 300 mg/day, pimozide 2 mg/day, escitalopram 40 mg/day, bupropion 300 mg/day, and lithium 600 mg/day (lithemia levels in range).
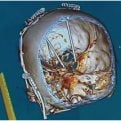
The implantation of the DBS system was performed according to standard techniques (2, 6, 9). A Leksell G-frame was applied to the patient’s head with local anesthesia and a computerized tomography (CT) scan was executed and merged with a previously performed T1 3D MRI, and rebuilt in axial, coronal, and sagittal planes. The target location was selected according to Hamani et al. (1) (see Fig. 1). Libra electrodes (St Jude Medical, Plano, TX, USA), consisting of a 3-mm distal contact and three 1-mm proximal contacts spaced 0.5 mm apart, were implanted at the planned targets and connected to bilateral Libra internal pulse generators (St Jude Medical). During the immediate postoperative period, the patient had a tonic – clonic seizure, which spontaneously subsided. A CT was quickly performed, which ruled out any intracranial hemorrhage. Three days following the procedure, a postoperative MRI was obtained. Despite the MRI quality being poor due to movement artefacts, it was sufficient to visualize the contact location.
On the first postoperative day, the patient and caregivers reported an improvement in her depression symptoms, which lasted for three days, after which she returned to her baseline. Stimulation was commenced 15 days after the operation, at the initial parameters proposed by Holtzeimer et al.
(2): 130 Hz, 91 l s, and 6 mA. Contacts were 3 – C + on the right side and 1 – C + on the left side, according to their position in the postoperative MRI, which showed that the right electrode was situated deeper than initially planned. From the first month of stimulation, the patient presented with a significant and progressive clinical response and normal functionality was restored. She began to autonomously perform home care tasks, and to engage in hobbies and pleasurable activities. Interestingly, despite her psychotic symptoms disappearing, some mild somatic perceptual distortions persisted, although their emotional impact was minimal.
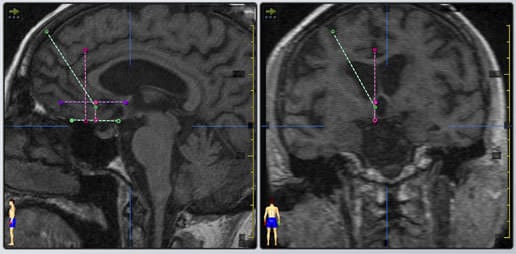
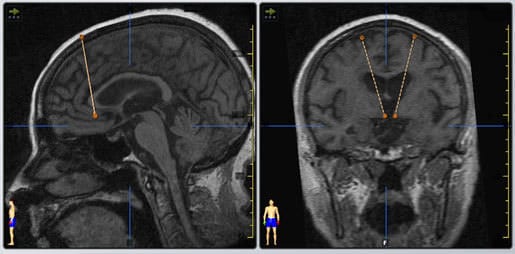
Fig. 1. Preoperative magnetic resonance (MR) imaging showing sagittal and coronal views of the planned subcallosal cingulated white matter target. (B) The final selected tracts for the subcallosal cingulated white matter deep brain stimulation implantation for medication-resistant type I bipolar depression.
These observations were supported by a significant reduction in her scores on the Hamilton Depression Rating Scale (HDRS), the Beck Depression Inventory, and the Montgomery-Asberg Depression Scale, and an increase in her Global Assessment Functioning scores, which persisted at the last follow-up at nine months (HDRS scores at baseline and at six and nine months of follow-up were 26, 13, and 7, respectively; see Fig. 2). Given the patient’s resistance to undergoing another MRI and the good clinical results, a second postoperative MRI was not performed. The stimulation parameters were not modified over her follow-up, and her medication was unchanged until the six-month follow-up, where it was gradually reduced to the current treatment: pimozide (1 mg/day), bupropion (150 mg/day), and lithium (600 mg/day). Seizures did not recur, and there were no complications related to the DBS. Her cognitive scores at the nine-month follow-up were unchanged.
No relapse of manic symptoms occurred, as reflected in her scores on the Young Mania Scale (Fig. 2). Some studies have suggested that the subcallosal cingulate might be an important structure involved in the pathophysiology of mania in patients with bipolar disorder (10). We believe that our results could offer new prospects for the treatment of patients with severe and otherwise refractory bipolar depression, and highlight the need for larger studies to determine whether DBS of the subcallosal cingulate is an effective and safe treatment for patients with refractory bipolar disorder (4)
.
DBS for type I bipolar depression
The authors of this paper do not have any commercial associations that might pose a conflict of interest in connection with this manuscript.
Cristina V Torres a , Elena Ezquiaga b , Marta Navas a and Rafael García de Sola: a Division of Neurosurgery, Department of Surgery, b Department of Psychiatry, University Hospital La Princesa, Madrid, Spain
Corresponding author:
Cristina V. Torres, MD, PhD Division of Neurosurgery Department of Surgery. University Hospital La Princesa. C/Diego de Le o n 32. 28006 Madrid Spain
Fax: (0034) 914013582
E-mail: cristinatorresdiaz@yahoo.es
doi: 10.1111/bdi.12102
© 2013 John Wiley and Sons A/S
Published by John Wiley and Sons Ltd.