¿Mejora la reintervención la supervivencia en el glioblastoma recurrente?
El glioblastoma recurrente, una forma agresiva de cáncer cerebral, plantea desafíos significativos en su tratamiento debido a su resistencia a la terapia estándar. A pesar de los avances en la investigación, su pronóstico sigue siendo sombrío, con una supervivencia promedio de solo unos meses. La recurrencia del glioblastoma se atribuye a la habilidad de las células cancerosas para evadir la destrucción y regenerarse. Los científicos están explorando nuevas estrategias terapéuticas, como la inmunoterapia y la terapia genética, en un esfuerzo por mejorar los resultados para los pacientes afectados por esta devastadora enfermedad.
Glioblastoma recurrente: Enfrentando un sesgo temporal en la literatura
Antecedentes
El glioblastoma (GBM) es el tumor cerebral maligno intraaxial más frecuente, en el que el tratamiento de la recidiva es un tema frecuente y exigente. Recientemente, la reintervención ha surgido como una herramienta útil para el tratamiento. Sin embargo, algunas nuevas pruebas han demostrado que la mayoría de los artículos publicados podrían haber sobrestimado sus efectos. Nuestro objetivo era analizar el efecto de la reintervención sobre la supervivencia considerándola una variable dependiente del tiempo y compararla con el análisis estadístico clásico.
Métodos
Realizamos un estudio retrospectivo con pacientes de GBM entre 2007 y 2017. Comparamos la supervivencia general (SG) entre los grupos de reintervención y los que no lo son con métodos estadísticos dependientes del tiempo (métodos de Simon-Makuch y de marcación y análisis Cox multivariable dependiente del tiempo) y los comparamos con los obtenidos con análisis de variables de tiempo no dependientes.
Resultados
Se incluyeron en el análisis un total de 183 pacientes y 44 de ellos fueron reoperados. El análisis estándar con Kaplan-Meier y la regresión multivariable de Cox de la cohorte mostró una SG de 22,2 meses (IC 95% 12,56-16,06) en el grupo de reintervención y 11,8 meses (IC 95% 9,87-13,67) en el grupo de no reintervención (p &l 0,001); y un CRI de 0,649 (IC 95% 0,434-0,97 p = 0,035) para la reintervención, demostrando un aumento de la SG. Sin embargo, el análisis dependiente del tiempo con la prueba de Simon-Makuch y el método de referencia mostró que la relación no era consistente, ya que este aumento de la SG no era significativo. Además, el análisis multivariable dependiente del tiempo de Cox no mostró que la reintervención mejorara la SG en nuestra cohorte (CRI 0,997 95% CI 0,976-1,018 p = 0,75).
Glioblastoma recurrente: Conclusiones
Ha habido un sesgo temporal en la literatura que ha llevado a una sobreestimación del efecto positivo de la reintervención en el GBM recurrente. Sin embargo, la reintervención podría seguir siendo útil en algunos pacientes seleccionados, que deberían ser individualizados según los factores de pronóstico relacionados con el paciente, la biología del tumor y las características del procedimiento quirúrgico.
Does reintervention improve survival in recurrent glioblastoma? Facing a temporal bias in the literature
- Juan Delgado-Fernández (ORCID: orcid.org/0000-0002-4251-83561),
Natalia Frade-Porto,
Guillermo Blasco,
Patricia González-Tarno,
Ricardo Gil-Simoes,
Zhi-Qiang Li,
Paloma Pulido Rivas &
Rafael García de Sola
Does reintervention improve survival in recurrent glioblastoma? Facing a temporal bias in the literature
Juan Delgado-Fern‡ndez (1) & Natalia Frade-Porto (2) & Guillermo Blasco (2) & Patricia Gonz‡lez-Tarno (2) &
Ricardo Gil-Simoes (2) & Zhi-Qiang Li (3) & Paloma Pulido Rivas (2) & Rafael García de Sola (4)
* Juan Delgado-Fern‡ndez juan.delgado.fdez@gmail.com
1 Department of Neurosurgery, University Hospital 12 de Octubre, Avda de C—rdoba S/N, 28041 Madrid, Spain
2 Division of Neurosurgery, Department of Surgery, University Hospital La Princesa, Madrid, Spain
3 Department of Neurosurgery, Zhongnan Hospital, Wuhan University, Wuhan, China
4 Innovation in Neurosurgery, Department of Neurosurgery, Hospital del Rosario, Universidad Autonoma de Madrid, Madrid, Spain
Received: 5 December 2019 / Accepted: 26 May 2020 / Published online: 16 June 2020
# Springer-Verlag GmbH Austria, part of Springer Nature 2020
Abstract.
Background Glioblastoma (GBM) is the most frequent intraaxial malignant brain tumour, in which recurrence management is a frequent and demanding issue. Recently, reintervention has emerged as a useful tool for treatment. However, some new evidence has shown that most of the articles published could have overestimated its effects. We aimed to analyse the effect on survival of reintervention considering it as a time-dependent variable and to compare it with classic statistical analysis.
Methods.
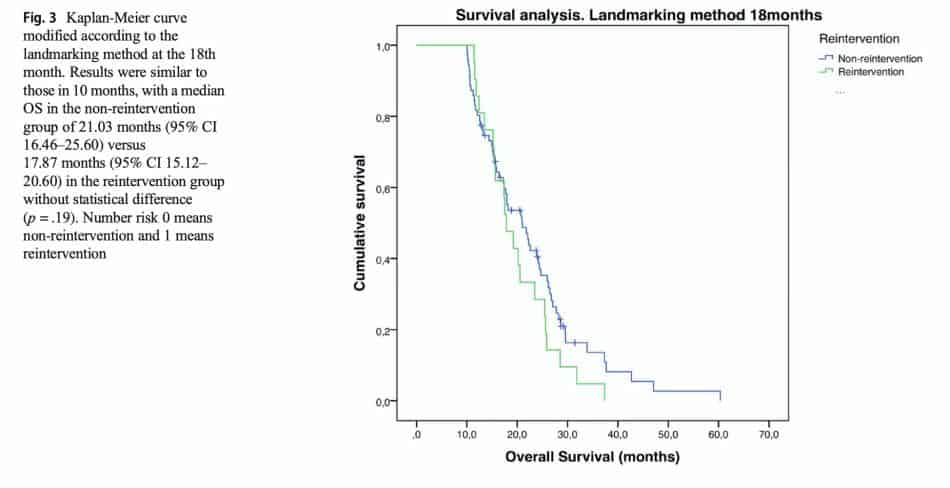
We performed a retrospective study with GBM patients between 2007 and 2017. We compared the overall survival (OS) between reintervention and non-reintervention groups with time-dependent statistical methods (Simon-Makuch and landmarking methods and time-dependent multivariable Cox analysis) and compared them with those obtained with nondependent time variable analysis.
Results.
A total of 183 patients were included in the analysis and 44 of them were reoperated. The standard analysis with KaplanMeier and multivariable Cox regression of the cohort showed an OS of 22.2 months (95% CI 12.56Ð16.06) in the reintervention group and 11.8 months (95% CI 9.87Ð13.67) in the non-reintervention group (p < .001); and an HR 0.649 (95% CI 0.434Ð0.97 p = .035) for reintervention, demonstrating an increase in OS. However, time-dependent analysis with the Simon-Makuch test and the landmarking method showed that the relationship was not consistent, as this increase in OS was not significant. Moreover, time-dependent multivariable Cox analysis did not show that reintervention improved OS in our cohort (HR 0.997 95% CI 0.976Ð1.018 p = 0.75).
Conclusions.
There has been a temporal bias in the literature that has led to an overestimation of the positive effect of reintervention in recurrent GBM. However, reintervention could still be useful in some selected patients, who should be individualized according to prognostic factors related to the patient, biology of the tumour, and characteristics of surgical procedure.
Keywords:
Glioblastoma, Recurrent glioblastoma, Reintervention, Survival, Temporal bias, Time-dependent statistical analysis.
Background
Glioblastoma (GBM) is the most frequent malignant primary brain tumour in adults and one of the most devastating tumours due to its poor prognosis. Firstly, GBM represents 47.7% of newly diagnosed gliomas with an incidence of 7 cases per 100,000 cases per year in the USA [21]. Secondly, survival is still very poor, with a mean survival with maximal therapy ranging from 12 to 15 months, and a 5-year survival rate of 5.6% [21, 28]. Moreover, in the last 25 years, despite the use of chemoradiotherapy, or other strategies such as angiogenesis inhibitors, targeted therapies, or gammaknife, the improvement in mean survival has increased only 3 months [19, 22, 33]. From the surgical point of view, some articles have described how maximal initial resection [20, 27, 34], and even supramarginal resection can increase survival in those patients [13]. Although this treatment is usually performed, GBM typically recurs during the first year [2, 30]. Due to this, different groups have demonstrated that reintervention could have an impact on the treatment of glioblastoma recurrence increasing overall survival (OS) independently of other prognostic factors [5, 14, 15, 30]. Some of these studies have led to the recommendation of reintervention in recurrent GBM, despite the low level of evidence [26]. Recently, Goldman et al. [10] published a case series where they found that there was not such a benefit in the patients that underwent reintervention. This was related to the so-called ÒsurvivalÓ or Òtime-dependent biasÓ. This bias is a well-known mistake in survival analysis that overestimates the effect of an intervention in a group of patients. This error has previously been described in oncology, leukaemia, and infectious patients or organ transplant [8, 9, 11]. In relation to this study, Zhao et al. [35], performed a meta-analysis, using time-dependent statistical tools and demonstrated that some previous articles have overestimated the OS of GBM patients undergoing reintervention due to time-dependent bias. To better understand this concept, the study by Gleiss et al. [9] exemplifies it by comparing survival related to graft failure in two groups of patients with a kidney transplant. At the initial point of transplantation, researches do not know which grafts will fail, neither at which point in the study, however, considering one of those patients as a graft failure since the transplantation will increase their survival, compromising the results, because this variable has not been considered as time-dependent. In our case, in the classical Kaplan-Meier test, GBM patients would be included as reoperated patients since the diagnosis if they eventually received a second intervention. However, the period from the diagnosis to second intervention would increase their OS although the patient did not receive this second procedure during this period. If we want to compare only the increased time of survival due to reintervention, we have to take into account the moment of the reintervention and the increased survival from this point. Therefore, if we do not treat reintervention as time-dependent, all patients that have a second surgery are considered from the very beginning in the reintervention group, and this could lead to an overestimation of their survival.
The objective of our study is, therefore, to perform an analysis of the survival of patients that underwent a second surgery and compared it with those who had not, using the reintervention as a time-dependent covariable and eliminating the survival bias, to elucidate if reintervention is indeed useful in the treatment of GBM recurrence.


