Do we need to wake patients up during Cortical Surgery?
1-Clinical Neurophysiology, Hospital Universitario de la Princesa, Madrid, Spain.
2-Instituto de Investigaciones Biomédicas del Hospital Universitario La Princesa, Madrid, Spain
3-Professor Emeritus of Neurosurgery, Universidad Autónoma de Madrid, Spain..
4-Hospital Nuestra Señora del Rosario, Madrid, Spain
5-Neurosurgery, Hospital Universitario de la Princesa, Madrid, Spain.
Abstract:
In recent years, a renewed fashion for awake surgery has appeared. In spite of its undoubted utility for scientific research, this technique has several limitations and flaws, usually not debated by parts of the scientific community.
We will discuss the aims and limitations of cortical surgery, especially the points relevant to protecting the patient. These objectives should define the guidelines that direct clinical practice. We will review the awake technique as well as various tools used in intraoperative neurophysiological monitoring (IONM) to explore and monitor several cortical functions during long surgeries. The main topics discussed include electrocorticography (ECoG) and cortically recorded evoked potentials (EP), including somatosensory, visual and auditory. Later, we will discuss methods to identify and survey motor functions as motor-evoked potentials, although they are elicited trans-cranially. Finally, we will briefly discuss a promising technique to monitor some language functions in anaesthetized patients, such as cortico-cortical evoked potentials (CCEP). We will address in depth some technical questions about electrical stimulation whose full relevance are not always considered.
Finally, we will discuss why, in the absence of empirical facts showing unequivocal superiority in post-surgical outcome, we have to awaken patients, especially when an alternate possibility exists without worst clinical results, as is the case for IONM.
Keywords: Anaesthetized surgery, awake surgery, cortical mapping, cortico-cortical evoked potentials, intraoperative neurophysiological monitoring.
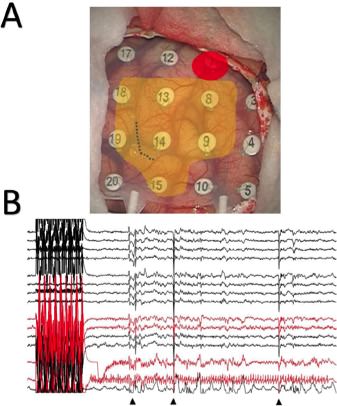
A) Image showing the cortical mapping results. Red: Wernicke’s area to 13 mA. Orange: region with negative results above 12 mA. The dotted line indicates the cortical incision for approaching the cavernoma.
B) Recording showing long-term after-discharges following stimulation by electrodes 18/1 to 9 mA. The widespread artefact (arrowhead) corresponds to the moment at which cool serum was administered. Subsequently, the discharges disappeared. The channels affected by after-discharges are shown in red.
INTRODUCTION
In recent years, there has been a renewed interest in surgery in awake patients [1-3]. This procedure uses the asleep-awake-sleep anaesthetic technique, which consists of induction with propofol + sevoflurane and topical blocking with svedocain + lidocaine around the skin incision. During exploration, the patient must be awoken slowly by removing the sedation. Recently, a new anaesthetic, dexmedetomidine, has been introduced for this type of surgery and is considered the most effective option [4], not only for asleep-awake- asleep technique, but for the conscious sedation one [5].
The scientific interest and relevance of this technique are undisputed. However, its clinical necessity is yet to be demonstrated, the surgery under total anaesthesia with intraoperative neurophysiological monitoring (IONM) is obviously more comfortable for both patients and medical staff. The main question that remains to be answered, therein, is whether the safety of the two techniques is equivalent.
Until now, no systematic comparison has been performed between awake and sedate craniotomy for cortical or subcortical surgery, and a definite answer remains to be established. However, both positions, for and against awake craniotomy, can be argued in this interesting debate, which is the topic of this work.
In our institutions, we have systematically performed IONM on anaesthetized patients for cortical and subcortical surgery for more than fifteen years, and we are firmly convinced of the validity of this approach.
IONM is a set of neurophysiological techniques that cannot evaluate complex functions (i.e., language function, visual or cognitive performance) but can allow the identification primary/eloquent structures with great confidence. Recently, even some parts of the language have been ascertained by cortico-cortical potentials in anaesthetised patients.
Our aim in this review is to show the powerful set of IONM techniques for use during cortical and subcortical surgery and to discuss why we think that a rational use of them can avoid the stress induced by awakening the patient.
…